
BRAIN DISEASES
With a dead brain, you're just a vessel.
ADHD - Attention Deficit Hyperactivity Disorder
DEFINITION
ADHD - Attention deficit hyperactivity disorder - Similar to hyperkinetic disorder in the ICD-10) is a developmental neuropsychiatric disorder in which there are significant problems with executive functions (e.g., attentional control and inhibitory control) that cause attention deficits, hyperactivity, or impulsiveness which is not appropriate for a person's age. These symptoms must begin by age six to twelve and persist for more than six months for a diagnosis to be made. In school-aged individuals inattention symptoms often result in poor school performance.
SYMPTOMS
Source: http://psychcentral.com/disorders/attention-deficit-hyperactivity-disorder-adhd-symptoms/
Several symptoms must be present before age 12 (which is why ADHD is classified as a neurodevelopmental disorder, even if not diagnosed until adulthood). In the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), symptoms were required before age 7. Now the age of 12 is seen as an acceptable criterion because it is often difficult for adults to look retrospectively and establish a precise age of onset for a child. Indeed, adult recall of childhood symptoms tends to be unreliable. Thus, the DSM-5 has added some leeway to the age cut-off.
A person can present with symptoms that are predominantly characterized by inattention, predominantly hyperactivity-impulsivity, or a combination of the two. To meet for each of these ADHD specifiers, a person must exhibit at least 6 symptoms from the appropriate categories below.
Symptoms of Inattention
Symptoms of Hyperactivity
Symptoms of Impulsivity
WHAT FACTORS CONTRIBUTE TO ADHD?
ADHD is a neurobehavioral disorder. According to the Centers for Disease Control and Prevention (CDC), about 5 percent of children in the United States have ADHD. It affects the way in which a person’s brain processes information and, in turn, influences behavior. The exact cause of ADHD is unknown. According to the Mayo Clinic, researchers believe that genetics, nutrition, brain development, and other factors play a significant role.
There is strong evidence that a person’s genes influence ADHD. In the few studies conducted with twins, researchers have consistently found that ADHD runs in families. It has been found to especially affect close relatives of people with ADHD. If your mother or father has ADHD, you and your siblings are more likely to have the disorder.
No one has yet been able to determine exactly which genes influence ADHD. Some studies have discovered a connection between ADHD and the DRD4 gene. Preliminary research indicates that this gene affects dopamine receptors in the brain. Some people with ADHD have a variation of this gene. This fact leads experts to believe it plays a role in the development of the condition. Still, researchers believe there is more than one gene responsible for ADHD.
It’s important to note that ADHD has been diagnosed in individuals who have no family history of the condition. A person’s environment and a combination of other factors can also influence whether or not you develop this disorder.
Exposure to organophosphate pesticides has also been linked to ADHD. These pesticides are chemicals sprayed on lawns and agricultural products. They include corn, apples, pears, grapes, berries, and peaches. Organophosphates are believed to disrupt the neurotransmitter acetylcholine in a child’s developing brain. This key neurotransmitter is responsible for controlling memory, attention, awareness, perception, reasoning, and judgment.
According to the Mayo Clinic, some studies suggest that certain food dyes and preservatives may cause hyperactivity in some children. Foods with artificial coloring include most processed and packaged snack foods. Sodium benzoate preservative is found in fruit pies, jams, soft drinks, and relishes. Researchers have not determined exactly how these ingredients influence ADHD, only that they appear to worsen its symptoms.
Perhaps the strongest link between the environment and ADHD occurs before a child is born. According to the CDC, prenatal exposure to smoking is associated with the behaviors of children with ADHD. Nicotine can affect the same dopamine receptors influenced by the DRD4 gene. A study published by the University of Nebraska suggests that children who were exposed to alcohol and drugs while in the womb were more likely to have ADHD.
There are many myths about what causes ADHD. Research has found no evidence that ADHD is caused by:
DIAGNOSIS
Source : http://www.webmd.com/add-adhd/guide/diagnosing-adhd
ADHD in Children
Health care providers, such as pediatricians, psychiatrists, and child psychologists, can diagnose ADHD with the help of standard guidelines from the American Academy of Pediatrics or the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM). The diagnosis involves gathering information from several sources, including schools, caregivers, and parents. The health care provider will consider how a child's behavior compares with that of other children the same age, and he or she may use standardized rating scales to document these behaviors.
To diagnose ADHD, your child should receive a full physical exam, including vision and hearing screenings. Also, the FDA has approved the use of the Neuropsychiatric EEG-Based Assessment Aid (NEBA) System, a noninvasive scan that measures theta and beta brain waves. The theta/beta ratio has been shown to be higher in children and adolescents with ADHD than in children without it. The scan, approved for use in those aged 6 to 17 years, is meant to be used as a part of a complete medical and psychological exam.
In addition, the health care provider should take a complete medical history to screen for other conditions that may affect a child's behavior. Certain conditions that could mimic ADHD or cause the ADHD-like behaviors are:
Recent major life changes (such as divorce, a death in the family, or a recent move)
TREATMENT
Pharmacology treatment
Source: http://www.caddra.ca/pdfs/caddraGuidelines2011Chapter07.pdf
Use principles of informed consent to ensure the patient is adequately educated when addressing
medication questions, particularly regarding degree of efficacy and side effects.
Non-pharmacological therapy
Source : http://www.adhd-institute.com/disease-management/non-pharmacological-therapy/
Non-pharmacological therapy links
ADHD - Attention deficit hyperactivity disorder - Similar to hyperkinetic disorder in the ICD-10) is a developmental neuropsychiatric disorder in which there are significant problems with executive functions (e.g., attentional control and inhibitory control) that cause attention deficits, hyperactivity, or impulsiveness which is not appropriate for a person's age. These symptoms must begin by age six to twelve and persist for more than six months for a diagnosis to be made. In school-aged individuals inattention symptoms often result in poor school performance.
SYMPTOMS
Source: http://psychcentral.com/disorders/attention-deficit-hyperactivity-disorder-adhd-symptoms/
Several symptoms must be present before age 12 (which is why ADHD is classified as a neurodevelopmental disorder, even if not diagnosed until adulthood). In the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), symptoms were required before age 7. Now the age of 12 is seen as an acceptable criterion because it is often difficult for adults to look retrospectively and establish a precise age of onset for a child. Indeed, adult recall of childhood symptoms tends to be unreliable. Thus, the DSM-5 has added some leeway to the age cut-off.
A person can present with symptoms that are predominantly characterized by inattention, predominantly hyperactivity-impulsivity, or a combination of the two. To meet for each of these ADHD specifiers, a person must exhibit at least 6 symptoms from the appropriate categories below.
Symptoms of Inattention
- Often fails to give close attention to details or makes careless mistakes in schoolwork, work, or other activities
- Often has difficulty sustaining attention in tasks or play activities
- Often does not seem to listen when spoken to directly
- Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (not due to oppositional behavior or failure to understand instructions)
- Often has difficulty organizing tasks and activities
- Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (such as schoolwork or homework)
- Often loses things necessary for tasks or activities (e.g., toys, school assignments, pencils, books, or tools)
- Is often easily distracted by extraneous stimuli
- Is often forgetful in daily activities–even those the person performs regularly (e.g., a routine appointment)
Symptoms of Hyperactivity
- Often fidgets with hands or feet or squirms in seat
- Often leaves seat in classroom or in other situations in which remaining seated is expected
- Often runs about or climbs excessively in situations in which it is inappropriate (in adolescents or adults, may be limited to subjective feelings of restlessness)
- Often has difficulty playing or engaging in leisure activities quietly
- Is often “on the go” or often acts as if “driven by a motor”
- Often talks excessively
Symptoms of Impulsivity
- Often blurts out answers before questions have been completed
- Often has difficulty awaiting turn
- Often interrupts or intrudes on others (e.g., butts into conversations or games)
- Symptoms must have persisted for at least 6 months. Some of these symptoms need to have been present as a child, at 12 years old or younger. The symptoms also must exist in at least two separate settings (for example, at school and at home). The symptoms should be creating significant impairment in social, academic or occupational functioning or relationships.
WHAT FACTORS CONTRIBUTE TO ADHD?
ADHD is a neurobehavioral disorder. According to the Centers for Disease Control and Prevention (CDC), about 5 percent of children in the United States have ADHD. It affects the way in which a person’s brain processes information and, in turn, influences behavior. The exact cause of ADHD is unknown. According to the Mayo Clinic, researchers believe that genetics, nutrition, brain development, and other factors play a significant role.
- Genes
There is strong evidence that a person’s genes influence ADHD. In the few studies conducted with twins, researchers have consistently found that ADHD runs in families. It has been found to especially affect close relatives of people with ADHD. If your mother or father has ADHD, you and your siblings are more likely to have the disorder.
No one has yet been able to determine exactly which genes influence ADHD. Some studies have discovered a connection between ADHD and the DRD4 gene. Preliminary research indicates that this gene affects dopamine receptors in the brain. Some people with ADHD have a variation of this gene. This fact leads experts to believe it plays a role in the development of the condition. Still, researchers believe there is more than one gene responsible for ADHD.
It’s important to note that ADHD has been diagnosed in individuals who have no family history of the condition. A person’s environment and a combination of other factors can also influence whether or not you develop this disorder.
- Neurotoxins
Exposure to organophosphate pesticides has also been linked to ADHD. These pesticides are chemicals sprayed on lawns and agricultural products. They include corn, apples, pears, grapes, berries, and peaches. Organophosphates are believed to disrupt the neurotransmitter acetylcholine in a child’s developing brain. This key neurotransmitter is responsible for controlling memory, attention, awareness, perception, reasoning, and judgment.
- Nutrition
According to the Mayo Clinic, some studies suggest that certain food dyes and preservatives may cause hyperactivity in some children. Foods with artificial coloring include most processed and packaged snack foods. Sodium benzoate preservative is found in fruit pies, jams, soft drinks, and relishes. Researchers have not determined exactly how these ingredients influence ADHD, only that they appear to worsen its symptoms.
- During Pregnancy
Perhaps the strongest link between the environment and ADHD occurs before a child is born. According to the CDC, prenatal exposure to smoking is associated with the behaviors of children with ADHD. Nicotine can affect the same dopamine receptors influenced by the DRD4 gene. A study published by the University of Nebraska suggests that children who were exposed to alcohol and drugs while in the womb were more likely to have ADHD.
- Myths
There are many myths about what causes ADHD. Research has found no evidence that ADHD is caused by:
- consuming excessive amounts of sugar
- TV watching
- video game playing
- poverty
- poor parenting
DIAGNOSIS
Source : http://www.webmd.com/add-adhd/guide/diagnosing-adhd
ADHD in Children
Health care providers, such as pediatricians, psychiatrists, and child psychologists, can diagnose ADHD with the help of standard guidelines from the American Academy of Pediatrics or the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM). The diagnosis involves gathering information from several sources, including schools, caregivers, and parents. The health care provider will consider how a child's behavior compares with that of other children the same age, and he or she may use standardized rating scales to document these behaviors.
To diagnose ADHD, your child should receive a full physical exam, including vision and hearing screenings. Also, the FDA has approved the use of the Neuropsychiatric EEG-Based Assessment Aid (NEBA) System, a noninvasive scan that measures theta and beta brain waves. The theta/beta ratio has been shown to be higher in children and adolescents with ADHD than in children without it. The scan, approved for use in those aged 6 to 17 years, is meant to be used as a part of a complete medical and psychological exam.
In addition, the health care provider should take a complete medical history to screen for other conditions that may affect a child's behavior. Certain conditions that could mimic ADHD or cause the ADHD-like behaviors are:
Recent major life changes (such as divorce, a death in the family, or a recent move)
- Undetected seizures
- Thyroid problems
- Sleep problems
- Anxiety
- Depression
- Lead toxicity
TREATMENT
Pharmacology treatment
Source: http://www.caddra.ca/pdfs/caddraGuidelines2011Chapter07.pdf
- STEP 1
Use principles of informed consent to ensure the patient is adequately educated when addressing
medication questions, particularly regarding degree of efficacy and side effects.
- STEP 2
- One central philosophy within CADDRA is to treat each patient as a unique being and to use the clinical advice within the “Seventeen Considerations for Medication Selection” as the guide.
- Practice Point: There are some practical questions that begin the selection process:
- Is medication indicated in your age group? Generally speaking, the first choice should be a medication that has an approved indication by Health Canada for ADHD within the specified age group. Even though some ADHD medications are not officially approved by Health Canada for a specific age group, doctors may decide to use them based on scientific evidence and expert consensus.
- What impairment do you have and at what time of the day? Is it mainly during work hours, meetings, exam times, leisure times, driving periods, morning routines, etc.? Ensure the patient is medicated when it is necessary and that you understand and are responding to his/her individual needs.
- What medication do you prefer? Have you ever taken any medications before or heard of something you might want to try? Patients respond better to the medications they most strongly believe in. This also addresses the belief that patients must be educated and they should have a partnership in the treatment agenda.
- Is a family member on medication for ADHD? If yes, then consider trying the same medication first. (Note: there is no evidence at this time about a possible role for such a pharmacogenetics-based approach.)
- Do you have third party coverage or do you plan to pay for the medication? Many of the current medications are expensive so there should be an open discussion related to government plans, third party insurance coverage, direct payment, co-payment plans and limited benefit plans.
- Do you have trouble swallowing a pill? If yes, then that will limit certain medications choices, though one should make an attempt to train the individual to swallow a capsule.
- Do you require urgent treatment? If yes, then a stimulant is likely your first choice due to its speed of onset of effect. However, the treatment of ADHD is a long-term plan so while there may be urgent issues, the patient should be cautioned about rapid fixes.
- Does the patient have comorbid disorders that require more complex interventions? If yes, the current agenda is to decide which problem to treat first. If it is ADHD, then initiate the ADHD medication and see what residual symptoms are left over that require further management. Anticipate drug-drug interaction issues. If the patient is expressing suicidal or homicidal thoughts these need to be addressed as a priority.
- STEP 3
- Establish a schedule for visits and contact with the patient and parents
- It is useful to establish an objective measure within the patient's domain. For example, the teacher may want to observe a five minute on-task behaviour. An adolescent may target their ability to sustain attention in their most difficult tasks. An adult may use a specific target that needs to change, like hourly work production. Formal observational rating scales help to quantify specific medication changes particularly at school and home. The CADDRA Clinician ADHD Baseline/Follow-up Form and the ADHD Checklist can be used to evaluate change
- During the titration phase, weekly contact with the patient reporting in either by phone, email, fax or visit is recommended. Ideally, the patient should be seen every two to three weeks where possible for a review of medication doses during the titration period and to check physical health, vital signs, review side effects, family functioning, patient and family well being, coping strategy management, behavioral treatment and other therapies when indicated.
- STEP 4
- Recommended starting dose and schedule for dose increases is a guide only.
- Start low and go slow but continue to increase the dose until the desired goals of treatment have been reached or side effects preclude dose increases. Optimal treatment means that the symptoms have decreased and that there is improvement in general functioning. Optimal dose is also that dose above which there is no further improvement. Sometimes side effects limit the dose titration . The threshold maximum suggestions in this document are consistent with the off-label standards established by the American Academy of Child and Adolescent Psychiatry.
- It is useful to alert the patient in advance that a peak effect may occur in the first week and a plateau effect may occur over the subsequent three weeks. Sometimes patients interpret this as a tolerance to the medication and request a higher dose. In fact, if the patient improves in their functioning at the plateau dose, they are likely dose-optimized.
- If there is an unsatisfactory response to one psychostimulant class, then there should be a switch to the other psychostimulant class.
- STEP 5
- In educating patients about medication it is important to provide the realistic view that individuals have different risk/benefit profiles on medication, ranging from those who cannot tolerate or benefit from medication at all, to those who have full remission with no side effects.
- While our evidence base on medication allows us to provide patients with a great deal of information on medication options, it is also important to remind patients and parents that all individuals are unique and may require doses that are smaller or larger than are usually recommended. It is important to point out that agreeing to a “trial” of medication is not a decision to use it forever. A trial is an experiment that carries minimal if any risks that would extend beyond a very brief period of time, and can be discontinued at any point.
- Patients who are good stimulant responders, but whose medication is limited by side effects, should be managed by the techniques described below or switched to a different medication regimen that minimizes that particular problem.
- Patients who are not responding to medication and obtaining little benefit, but do not have major side effects, may require non-medication strategies.
- If the patient does not respond to any of the first line medications, augmentation strategies or use ofsecond line medications such as guanfacine XR, third line options like buproprion, clonidine, modafinil or imipramine may be helpful, but a specialist referral should be made. In the rapidly changing field of ADHD, treatment with new medications with different side effect profiles and possibly differential effectiveness in particular patients is becoming possible.
- If a change in medication is thought necessary, switch medication during long vacations or during the summer to avoid possible side effects that may impair school performance in the short-term. However, sometimes switching medications requires a more immediate intervention due to the urgency of the situation.
- If a period off medication or on a reduced dose to minimize side effect is required, it should be done during long vacations, the summer, or on long weekends to minimize impact on school performance. Clinically, it is observed that interrupting medication every weekend may in fact increase side effects. Taking the medication each day will help develop a tolerance toward side effects. Some medications need to be taken continuously to maintain clinical effect. These medications should be tapered due to the risk of significant side effects or dangers
Non-pharmacological therapy
Source : http://www.adhd-institute.com/disease-management/non-pharmacological-therapy/
Non-pharmacological therapy links
- Behavioural therapy
- Psychoeducation
- Lifestyle & diet
EPILEPSY

DEFINITION
A central nervous system disorder (neurological disorder) in which nerve cell activity in the brain becomes disrupted, uncontrolled and abnormal, causing seizures or periods of unusual behavior, sensations and sometimes loss of consciousness. Epilepsy is the fourth most common neurological disorder and affects people of all ages. It means the same thing as "seizure disorders". In addition, epilepsy is characterized by unpredictable seizures and can cause other health problems. It is a spectrum condition with a wide range of seizure types and control varying from person-to-person,
SIGNS AND SYMPTOMS
CAUSES AND RISK FACTORS
Epilepsy occurs when there are permanent changes in the brain which cause the brain to be too excitable or irritable. As a result, the brain sends out abnormal signals. This leads to repeated, unpredictable seizures.
Source:
https://www.nlm.nih.gov/medlineplus/ency/article/000694.htm
http://www.mayoclinic.org/diseases-conditions/epilepsy/home/ovc-20117206
Common causes of epilepsy include:
-Abnormal levels of sodium or glucose in the blood
-Abnormal blood vessels in the brain
-Brain injury that occurs to the baby during labour or childbirth
-Brain problems that occur before birth (congenital brain defects: abnormality in the brain that are present at birth)
-Traumatic head injury
RISK FACTORS
Source: http://www.epilepsy.com/learn/epilepsy-101/what-are-risk-factors
- Babies who are born small for their age
- Serious brain injury or lack of oxygen to the brain
- Brain tumours
- Infections of the brain: abscess (swollen area within body tissue, containing an accumulation of pus), meningitis (inflammation of the meninges caused by viral or bacterial infection and marked by intense headache and fever, sensitivity to light, and muscular rigidity), or encephalitis (inflammation of the brain)
-Use of illegal drugs such as cocaine
DIAGNOSIS
Source: https://www.epilepsysociety.org.uk/tests-epilepsy#.VzqMlTV97bg
Diagnosing epilepsy is not simple. Doctors gather lots of different information to assess the causes of seizures. If you have had two or more seizures that started in the brain you may be diagnosed with epilepsy. Getting a diagnosis is not always easy as there is no single test that can diagnose epilepsy. If there is a possibility that you have epilepsy, NICE recommends that you are referred to a specialist, (a doctor who is trained in diagnosing and treating epilepsy) within two weeks.
Your diagnosis is based on finding out what happened to you before, during and after your seizures. For example, some types of faints can look like epileptic seizures, and often before fainting a person feels cold, clammy and their vision goes blurry. But epileptic seizures happen very suddenly and a person may have no warning that a seizure is about to happen.
Blood tests, an Electroencephalogram (EEG) and scans are used to gather information for a diagnosis. Tests on their own cannot confirm or rule out epilepsy.
Blood tests
A sample of blood will usually be taken from your arm with a syringe. The sample is used to check your general health and to rule out other possible causes for your seizures, such as low blood sugar levels or diabetes.
Electrocardiogram (ECG)
An ECG is used to record the electrical activity of the heart. This is done by sticking electrodes (a bit like plasters) to the arms, legs and chest. These electrodes pick up the electrical signals from the heart.
An ECG does not give out electrical signals, so having one doesn’t hurt. An ECG can help to rule out the seizure being caused by the way the heart is working.
TREATMENT
The type of treatment prescribed will depend on several factors, including the frequency and severity of the seizures and the person's age, overall health, and medical history.
Below are a few examples of treatments:
Non- pharmacological
The Ketogenic Diet
The ketogenic diet is one of the oldest treatments for epilepsy. It is intended to maintain the starvation or fasting over a long period of time. When the body is in a fasting state, it creates ketones, a by-product of fat-burning metabolism. It has long been recognized that seizures often lessen or disappear during periods of fasting in some individuals with epilepsy.
The diet is very high in fat and low in carbohydrates. When fat is the primary source of calories, ketones are formed. The diet must be followed very strictly and requires a significant commitment to work effectively.
Pharmacological
Carbamazepine (Tegretol or Carbatrol)
A central nervous system disorder (neurological disorder) in which nerve cell activity in the brain becomes disrupted, uncontrolled and abnormal, causing seizures or periods of unusual behavior, sensations and sometimes loss of consciousness. Epilepsy is the fourth most common neurological disorder and affects people of all ages. It means the same thing as "seizure disorders". In addition, epilepsy is characterized by unpredictable seizures and can cause other health problems. It is a spectrum condition with a wide range of seizure types and control varying from person-to-person,
SIGNS AND SYMPTOMS
- Symptoms vary from person to person. Some people may have simple staring spells, where the patients stop what they're doing, lose eye-contact with other people, and appear to stare into space. Others have violent shaking and loss of alertness. The symptoms depend on the part of the brain that is affected.
- Some people with epilepsy have a strange sensation before each seizure. Sensations may be tingling, smelling an odour that is not actually there, or emotional changes.
CAUSES AND RISK FACTORS
Epilepsy occurs when there are permanent changes in the brain which cause the brain to be too excitable or irritable. As a result, the brain sends out abnormal signals. This leads to repeated, unpredictable seizures.
Source:
https://www.nlm.nih.gov/medlineplus/ency/article/000694.htm
http://www.mayoclinic.org/diseases-conditions/epilepsy/home/ovc-20117206
Common causes of epilepsy include:
-Abnormal levels of sodium or glucose in the blood
-Abnormal blood vessels in the brain
-Brain injury that occurs to the baby during labour or childbirth
-Brain problems that occur before birth (congenital brain defects: abnormality in the brain that are present at birth)
-Traumatic head injury
RISK FACTORS
Source: http://www.epilepsy.com/learn/epilepsy-101/what-are-risk-factors
- Babies who are born small for their age
- Serious brain injury or lack of oxygen to the brain
- Brain tumours
- Infections of the brain: abscess (swollen area within body tissue, containing an accumulation of pus), meningitis (inflammation of the meninges caused by viral or bacterial infection and marked by intense headache and fever, sensitivity to light, and muscular rigidity), or encephalitis (inflammation of the brain)
-Use of illegal drugs such as cocaine
DIAGNOSIS
Source: https://www.epilepsysociety.org.uk/tests-epilepsy#.VzqMlTV97bg
Diagnosing epilepsy is not simple. Doctors gather lots of different information to assess the causes of seizures. If you have had two or more seizures that started in the brain you may be diagnosed with epilepsy. Getting a diagnosis is not always easy as there is no single test that can diagnose epilepsy. If there is a possibility that you have epilepsy, NICE recommends that you are referred to a specialist, (a doctor who is trained in diagnosing and treating epilepsy) within two weeks.
Your diagnosis is based on finding out what happened to you before, during and after your seizures. For example, some types of faints can look like epileptic seizures, and often before fainting a person feels cold, clammy and their vision goes blurry. But epileptic seizures happen very suddenly and a person may have no warning that a seizure is about to happen.
Blood tests, an Electroencephalogram (EEG) and scans are used to gather information for a diagnosis. Tests on their own cannot confirm or rule out epilepsy.
Blood tests
A sample of blood will usually be taken from your arm with a syringe. The sample is used to check your general health and to rule out other possible causes for your seizures, such as low blood sugar levels or diabetes.
Electrocardiogram (ECG)
An ECG is used to record the electrical activity of the heart. This is done by sticking electrodes (a bit like plasters) to the arms, legs and chest. These electrodes pick up the electrical signals from the heart.
An ECG does not give out electrical signals, so having one doesn’t hurt. An ECG can help to rule out the seizure being caused by the way the heart is working.
TREATMENT
The type of treatment prescribed will depend on several factors, including the frequency and severity of the seizures and the person's age, overall health, and medical history.
Below are a few examples of treatments:
Non- pharmacological
The Ketogenic Diet
The ketogenic diet is one of the oldest treatments for epilepsy. It is intended to maintain the starvation or fasting over a long period of time. When the body is in a fasting state, it creates ketones, a by-product of fat-burning metabolism. It has long been recognized that seizures often lessen or disappear during periods of fasting in some individuals with epilepsy.
The diet is very high in fat and low in carbohydrates. When fat is the primary source of calories, ketones are formed. The diet must be followed very strictly and requires a significant commitment to work effectively.
Pharmacological
Carbamazepine (Tegretol or Carbatrol)
- anticonvulsant and specific analgesic for trigeminal neuralgia, available for oral administration
- anti-epileptic medication, also called an anticonvulsant.
- anticonvulsant
ISCHEMIC STROKE
Source: https://www.nlm.nih.gov/medlineplus/ency/article/000726.htm
DEFINITION
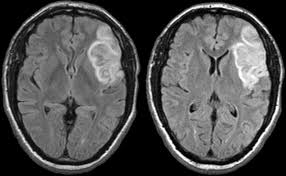
A stroke occurs when blood flow to a part of the brain stops. A stroke is sometimes called a "brain attack." If blood flow is cut off for longer than a few seconds, the brain cannot get nutrients and oxygen. Brain cells can die, causing lasting damage. An ischemic stroke occurs when a cerebral vessel occludes, obstructing blood flow to a portion of the brain
SIGNS AND SYMPTOMS
Symptoms of stroke depend on which part of the brain is damaged. In some cases, a person may not know that a stroke has occurred.
Most of the time, symptoms develop suddenly and without warning. But symptoms may occur on and off for the first day or two. Symptoms are usually most severe when the stroke first happens, but they may slowly get worse.
-Change in alertness (including sleepiness, unconsciousness, and coma)
-Changes in hearing or taste
-Changes that affect touch and the ability to feel pain, pressure, or different temperatures
-Confusion or loss of memory
-Problems swallowing
-Problems writing or reading
-Dizziness or abnormal feeling of movement (vertigo)
-Eyesight problems, such as decreased vision, double vision, or total loss of vision
-Lack of control over the bladder or bowels
CAUSES AND RISK FACTORS
Ischemic stroke occurs when a blood vessel that supplies blood to the brain is blocked by a blood clot. This may happen in two ways:
-A clot may form in an artery that is already very narrow. This is called a thrombotic stroke.
-A clot may break off from another place in the blood vessels of the brain, or from some other part of the body, and travel up to the brain. This is called cerebral embolism, or an embolic stroke.
Stroke risk is higher in:
-People who have heart disease or poor blood flow in their legs caused by narrowed arteries
-People who have unhealthy lifestyle habits such as smoking, a high-fat diet, and lack of exercise
-Women who take birth control pills (especially those who smoke and are older than 35)
-Women have an increased risk while pregnant
-Women who take hormone replacement therapy
DEFINITION
A stroke occurs when blood flow to a part of the brain stops. A stroke is sometimes called a "brain attack." If blood flow is cut off for longer than a few seconds, the brain cannot get nutrients and oxygen. Brain cells can die, causing lasting damage. An ischemic stroke occurs when a cerebral vessel occludes, obstructing blood flow to a portion of the brain
SIGNS AND SYMPTOMS
Symptoms of stroke depend on which part of the brain is damaged. In some cases, a person may not know that a stroke has occurred.
Most of the time, symptoms develop suddenly and without warning. But symptoms may occur on and off for the first day or two. Symptoms are usually most severe when the stroke first happens, but they may slowly get worse.
-Change in alertness (including sleepiness, unconsciousness, and coma)
-Changes in hearing or taste
-Changes that affect touch and the ability to feel pain, pressure, or different temperatures
-Confusion or loss of memory
-Problems swallowing
-Problems writing or reading
-Dizziness or abnormal feeling of movement (vertigo)
-Eyesight problems, such as decreased vision, double vision, or total loss of vision
-Lack of control over the bladder or bowels
CAUSES AND RISK FACTORS
Ischemic stroke occurs when a blood vessel that supplies blood to the brain is blocked by a blood clot. This may happen in two ways:
-A clot may form in an artery that is already very narrow. This is called a thrombotic stroke.
-A clot may break off from another place in the blood vessels of the brain, or from some other part of the body, and travel up to the brain. This is called cerebral embolism, or an embolic stroke.
Stroke risk is higher in:
-People who have heart disease or poor blood flow in their legs caused by narrowed arteries
-People who have unhealthy lifestyle habits such as smoking, a high-fat diet, and lack of exercise
-Women who take birth control pills (especially those who smoke and are older than 35)
-Women have an increased risk while pregnant
-Women who take hormone replacement therapy
DIAGNOSIS
-Physical examination.
-Blood tests.
-Computerized tomography (CT) scan.
-Magnetic resonance imaging (MRI).
TREATMENT
Pharmacological
-Anticoagulation
Non-pharmacological
-Physical examination.
- Your doctor will ask you or a family member what symptoms you've been having, when they started and what you were doing when they began. Your doctor then will evaluate whether these symptoms are still present.
- Your doctor will want to know what medications you take and whether you have experienced any head injuries. You'll be asked about your personal and family history of heart disease, transient ischemic attack or stroke.
- Your doctor will check your blood pressure and use a stethoscope to listen to your heart and to listen for a whooshing sound (bruit) over your neck (carotid) arteries, which may indicate atherosclerosis. Your doctor may also use an ophthalmoscope to check for signs of tiny cholesterol crystals or clots in the blood vessels at the back of your eyes.
-Blood tests.
- You may have several blood tests, which tell your care team how fast your blood clots, whether your blood sugar is abnormally high or low, whether critical blood chemicals are out of balance, or whether you may have an infection. Managing your blood's clotting time and levels of sugar and other key chemicals will be part of your stroke care.
-Computerized tomography (CT) scan.
- A CT scan uses a series of X-rays to create a detailed image of your brain. A CT scan can show a hemorrhage, tumor, stroke and other conditions. Doctors may inject a dye into your bloodstream to view your blood vessels in your neck and brain in greater detail (computerized tomography angiography).
-Magnetic resonance imaging (MRI).
- An MRI uses powerful radio waves and magnets to create a detailed view of your brain. An MRI can detect brain tissue damaged by an ischemic stroke and brain hemorrhages. Your doctor may inject a dye into a blood vessel to view the arteries and veins and highlight blood flow (magnetic resonance angiography, or magnetic resonance venography).
TREATMENT
Pharmacological
-Anticoagulation
- a class of drugs that work to prevent blood coagulation (clotting)
- restores blood flow through blocked arteries
- a class of pharmaceuticals that decrease platelet aggregation [1] and inhibit thrombus formation. They are effective in the arterial circulation, where anticoagulants have little effect
Non-pharmacological
- no implications on the effectiveness of non-pharmacological interventions post-stroke can be drawn
ALZHEIMER'S DISEASE
DEFINITION
Source: http://www.alz.org/research/science/alzheimers_research.asp
Alzheimer's disease is a progressive brain disorder that damages and eventually destroys brain cells, leading to memory loss and changes in thinking and other brain functions. It usually develops slowly and gradually gets worse as brain function declines and brain cells eventually wither and die. Ultimately, Alzheimer's is fatal, and currently, there is no cure.
SIGNS AND SYMPTOMS
Source: http://www.nhs.uk/Conditions/Alzheimers-disease/Pages/Symptoms.aspx
Source: http://www.alz.org/research/science/alzheimers_research.asp
Alzheimer's disease is a progressive brain disorder that damages and eventually destroys brain cells, leading to memory loss and changes in thinking and other brain functions. It usually develops slowly and gradually gets worse as brain function declines and brain cells eventually wither and die. Ultimately, Alzheimer's is fatal, and currently, there is no cure.
SIGNS AND SYMPTOMS
Source: http://www.nhs.uk/Conditions/Alzheimers-disease/Pages/Symptoms.aspx

Stages of Alzheimer's disease
Generally, the symptoms of Alzheimer's disease are divided into three main stages.
Early symptoms
In the early stages, the main symptom of Alzheimer's disease is memory lapses. For example, someone with early Alzheimer's disease may:
-forget about recent conversations or events, or misplace items
-forget the names of places and objects, or have trouble thinking of the right word
-repeat themselves regularly, such as asking the same question several times
-show poor judgement or find it harder to make decisions
-become less flexible and more hesitant to try new things
There are often signs of mood changes, such as increasing anxiety or agitation, or periods of confusion.
Middle-stage symptoms
As Alzheimer's disease develops, memory problems will get worse. Someone with the condition may find it increasingly difficult to remember the names of people they know and may struggle to recognise their family and friends.
Other symptoms may also develop, such as:
-increasing confusion and disorientation – for example, getting lost, or wandering and not knowing what time of day it is
-obsessive, repetitive or impulsive behaviour
-delusions (believing things that are untrue) or feeling paranoid and suspicious about carers or family members
-problems with speech or language (aphasia)
-disturbed sleep
-changes in mood, such as frequent mood swings, depression and feeling increasingly anxious, frustrated or agitated
-difficulty performing spatial tasks, such as judging distances
-hallucinations
By this stage, someone with Alzheimer's disease usually needs support to help them with their everyday living. For example, they may need help eating, washing, getting dressed and using the toilet.
Later symptoms
In the later stages of Alzheimer's disease, the symptoms become increasingly severe and distressing for the person with the condition, as well as their carers, friends and family.
Hallucinations and delusions may come and go over the course of the illness, but can get worse as the condition progresses. Sometimes people with Alzheimer's disease can be violent, demanding and suspicious of those around them.
A number of other symptoms may also develop as Alzheimer's disease progresses, such as:
-difficulty eating and swallowing (dysphagia)
-difficulty changing position or moving around without assistance
-considerable weight loss – although some people eat too much and put on weight
-unintentional passing of urine (urinary incontinence) or stools (bowel incontinence)
-gradual loss of speech
-significant problems with short- and long-term memory
In the severe stages of Alzheimer's disease, people may need full-time care and assistance with eating, moving and using the toilet.
CAUSES AND RISK FACTORS
Source: http://www.webmd.com/alzheimers/guide/alzheimers-causes-risk-factors
Generally, the symptoms of Alzheimer's disease are divided into three main stages.
Early symptoms
In the early stages, the main symptom of Alzheimer's disease is memory lapses. For example, someone with early Alzheimer's disease may:
-forget about recent conversations or events, or misplace items
-forget the names of places and objects, or have trouble thinking of the right word
-repeat themselves regularly, such as asking the same question several times
-show poor judgement or find it harder to make decisions
-become less flexible and more hesitant to try new things
There are often signs of mood changes, such as increasing anxiety or agitation, or periods of confusion.
Middle-stage symptoms
As Alzheimer's disease develops, memory problems will get worse. Someone with the condition may find it increasingly difficult to remember the names of people they know and may struggle to recognise their family and friends.
Other symptoms may also develop, such as:
-increasing confusion and disorientation – for example, getting lost, or wandering and not knowing what time of day it is
-obsessive, repetitive or impulsive behaviour
-delusions (believing things that are untrue) or feeling paranoid and suspicious about carers or family members
-problems with speech or language (aphasia)
-disturbed sleep
-changes in mood, such as frequent mood swings, depression and feeling increasingly anxious, frustrated or agitated
-difficulty performing spatial tasks, such as judging distances
-hallucinations
By this stage, someone with Alzheimer's disease usually needs support to help them with their everyday living. For example, they may need help eating, washing, getting dressed and using the toilet.
Later symptoms
In the later stages of Alzheimer's disease, the symptoms become increasingly severe and distressing for the person with the condition, as well as their carers, friends and family.
Hallucinations and delusions may come and go over the course of the illness, but can get worse as the condition progresses. Sometimes people with Alzheimer's disease can be violent, demanding and suspicious of those around them.
A number of other symptoms may also develop as Alzheimer's disease progresses, such as:
-difficulty eating and swallowing (dysphagia)
-difficulty changing position or moving around without assistance
-considerable weight loss – although some people eat too much and put on weight
-unintentional passing of urine (urinary incontinence) or stools (bowel incontinence)
-gradual loss of speech
-significant problems with short- and long-term memory
In the severe stages of Alzheimer's disease, people may need full-time care and assistance with eating, moving and using the toilet.
CAUSES AND RISK FACTORS
Source: http://www.webmd.com/alzheimers/guide/alzheimers-causes-risk-factors

-Age. Your risk for Alzheimer's goes up as you get older. For most people, it starts going up after age 65.
-Gender. Women get the disease more often than men.
-Family history. People who have a parent or sibling with Alzheimer’s are more likely to get it themselves.
-Down syndrome . It’s not clear why, but people with this disorder often get Alzheimer's disease in their 30s and 40s.
-Head injury. Some studies have shown a link between Alzheimer's disease and a major head injury.
-Other factors: High cholesterol levels and high blood pressure may also raise your risk.
DIAGNOSIS
Source: https://www.nia.nih.gov/alzheimers/topics/diagnosis
To diagnose Alzheimer’s, doctors may:
-Ask the person and a family member or friend questions about overall health, past medical problems, ability to carry out daily activities, and changes in behavior and personality
-Conduct tests of memory, problem solving, attention, counting, and language
-Carry out standard medical tests, such as blood and urine tests, to identify other possible causes of the problem
-Perform brain scans, such as computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET), to rule out other possible causes for symptoms.
TREATMENT
Pharmacological
There are two types of medication used to treat Alzheimer's disease: acetylcholinesterase inhibitors (often shortened to just 'cholinesterase inhibitors') and NMDA receptor antagonists. The two types work in different ways. These are explained below.
The generic names for the cholinesterase inhibitors are donepezil, rivastigmine and galantamine:
-Donepezil was originally patented as the brand name Aricept, but is more widely available now as just generic donepezil.
-Rivastigmine was patented as Exelon and is now also available as other brands, as well as generic rivastigmine.
-Galantamine was patented as Reminyl and is now also available as generic galantamine and the brands Reminyl XL, Acumor XL, Galsya XL and Gatalin XL.
The NMDA receptor antagonist is memantine. It was originally patented as Ebixa and is now also available as generic memantine. Other UK brand names for memantine include Maruxa and Nemdatine.
-Gender. Women get the disease more often than men.
-Family history. People who have a parent or sibling with Alzheimer’s are more likely to get it themselves.
-Down syndrome . It’s not clear why, but people with this disorder often get Alzheimer's disease in their 30s and 40s.
-Head injury. Some studies have shown a link between Alzheimer's disease and a major head injury.
-Other factors: High cholesterol levels and high blood pressure may also raise your risk.
DIAGNOSIS
Source: https://www.nia.nih.gov/alzheimers/topics/diagnosis
To diagnose Alzheimer’s, doctors may:
-Ask the person and a family member or friend questions about overall health, past medical problems, ability to carry out daily activities, and changes in behavior and personality
-Conduct tests of memory, problem solving, attention, counting, and language
-Carry out standard medical tests, such as blood and urine tests, to identify other possible causes of the problem
-Perform brain scans, such as computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET), to rule out other possible causes for symptoms.
TREATMENT
Pharmacological
There are two types of medication used to treat Alzheimer's disease: acetylcholinesterase inhibitors (often shortened to just 'cholinesterase inhibitors') and NMDA receptor antagonists. The two types work in different ways. These are explained below.
The generic names for the cholinesterase inhibitors are donepezil, rivastigmine and galantamine:
-Donepezil was originally patented as the brand name Aricept, but is more widely available now as just generic donepezil.
-Rivastigmine was patented as Exelon and is now also available as other brands, as well as generic rivastigmine.
-Galantamine was patented as Reminyl and is now also available as generic galantamine and the brands Reminyl XL, Acumor XL, Galsya XL and Gatalin XL.
The NMDA receptor antagonist is memantine. It was originally patented as Ebixa and is now also available as generic memantine. Other UK brand names for memantine include Maruxa and Nemdatine.
PSYCHOTIC DEPRESSION

Source: http://www.webmd.com/depression/guide/psychotic-depression
DEFINITION
Psychotic depression is a mental disorder which is a subtype of major depression that occurs when a severe depressive illness includes some form of psychosis. The psychosis could be hallucinations (such as hearing a voice telling you that you are no good or worthless), delusions (such as, intense feelings of worthlessness, failure, or having committed a sin) or some other break with reality. Psychotic depression affects roughly one out of every four people admitted to the hospital for depression.
SIGNS AND SYMPTOMS
A person with psychosis may have any of the following:
-Disorganized thought and speech
-False beliefs that are not based in reality (delusions), especially unfounded fear or suspicion
-Thoughts that "jump" between unrelated topics (disordered thinking)
-Observable severe depressed mood
-Severe social impairment
-Severe psychomotor disturbance (agitation, retardation, cognitive processing problems)
-Psychotic features such as delusions and/or hallucinations.
CAUSES AND RISK FACTORS
Source: https://www.nlm.nih.gov/medlineplus/ency/article/001553.htm
Medical problems that can cause psychotic depression include:
-Alcohol and certain illegal drugs, both during use and during withdrawal
-Brain diseases, such as Parkinson disease, Huntington disease
-Brain tumours or cysts
-Dementia (including Alzheimer’s disease)
-HIV and other infections that affect the brain
-Some prescription drugs, such as steroids and stimulants
-Epilepsy
-Stroke
People with higher risk to get psychotic depression:
DIAGNOSIS
http://www.blackdoginstitute.org.au/healthprofessionals/depression/ourmodelofdepression/psychoticdepression.cfm
TREATMENT
In psychotic depressions, hospitalisation may be indicated. ECT is very effective in treating psychotic depression – and is often the treatment of first choice, particularly if used successfully in previous episodes. It is not the option of last resort. If ECT is not appropriate, the treatment is a ‘broad-action’ antidepressant in
combination with an atypical antipsychotic. It is advised patients routinely take Omega-3 in conjunction with the medication. The antidepressant may be ‘dual-action' (SNRI) or ‘broader-action’ (TCA). If the combination of SNRI and antipsychotic is of insufficient benefit, the next medication option is (after an adequate wash-out period) to change the SNRI to a TCA.
Once the psychotic features have lifted, antipsychotic medication may be gradually ceased (continuation can be associated with significant side-effects). The antidepressant is usually required for an extended period. Ensure there have been therapeutic levels of the medication for an adequate period of time before deciding that medication has not been successful and moving on to ECT.
Non-pharmacological
In the early stages, psychotherapy is generally of little benefit. It may be useful at a later stage to explore impact on work and family and other recovery issues. There may be a place for CBT for depression, anxiety management and understanding personality style. Examination of issues and working on self-management strategies are important in preventing future depression, improving resilience and maximising the individual’s psychological wellbeing.
DEFINITION
Psychotic depression is a mental disorder which is a subtype of major depression that occurs when a severe depressive illness includes some form of psychosis. The psychosis could be hallucinations (such as hearing a voice telling you that you are no good or worthless), delusions (such as, intense feelings of worthlessness, failure, or having committed a sin) or some other break with reality. Psychotic depression affects roughly one out of every four people admitted to the hospital for depression.
SIGNS AND SYMPTOMS
A person with psychosis may have any of the following:
-Disorganized thought and speech
-False beliefs that are not based in reality (delusions), especially unfounded fear or suspicion
-Thoughts that "jump" between unrelated topics (disordered thinking)
-Observable severe depressed mood
-Severe social impairment
-Severe psychomotor disturbance (agitation, retardation, cognitive processing problems)
-Psychotic features such as delusions and/or hallucinations.
CAUSES AND RISK FACTORS
Source: https://www.nlm.nih.gov/medlineplus/ency/article/001553.htm
Medical problems that can cause psychotic depression include:
-Alcohol and certain illegal drugs, both during use and during withdrawal
-Brain diseases, such as Parkinson disease, Huntington disease
-Brain tumours or cysts
-Dementia (including Alzheimer’s disease)
-HIV and other infections that affect the brain
-Some prescription drugs, such as steroids and stimulants
-Epilepsy
-Stroke
People with higher risk to get psychotic depression:
- people with schizophrenia (a long-term mental disorder of a type involving a breakdown in the relation between thought, emotion, and behaviour, leading to faulty perception, inappropriate actions and feelings, withdrawal from reality and personal relationships into fantasy and delusion, and a sense of mental fragmentation)
- people with bipolar disorder (manic-depressive) or severe depression
- people with personality disorders
DIAGNOSIS
http://www.blackdoginstitute.org.au/healthprofessionals/depression/ourmodelofdepression/psychoticdepression.cfm
- Psychotic features: consistent with mood (mood congruent) or mood incongruent. Delusions more common than hallucinations (90% vs. 10%).
- Pathological guilt: common in psychotic depression
- Psychomotor disturbance: profound
- Cognitive function: mild cognitive processing problems through to pseudo-dementia.
TREATMENT
In psychotic depressions, hospitalisation may be indicated. ECT is very effective in treating psychotic depression – and is often the treatment of first choice, particularly if used successfully in previous episodes. It is not the option of last resort. If ECT is not appropriate, the treatment is a ‘broad-action’ antidepressant in
combination with an atypical antipsychotic. It is advised patients routinely take Omega-3 in conjunction with the medication. The antidepressant may be ‘dual-action' (SNRI) or ‘broader-action’ (TCA). If the combination of SNRI and antipsychotic is of insufficient benefit, the next medication option is (after an adequate wash-out period) to change the SNRI to a TCA.
Once the psychotic features have lifted, antipsychotic medication may be gradually ceased (continuation can be associated with significant side-effects). The antidepressant is usually required for an extended period. Ensure there have been therapeutic levels of the medication for an adequate period of time before deciding that medication has not been successful and moving on to ECT.
Non-pharmacological
In the early stages, psychotherapy is generally of little benefit. It may be useful at a later stage to explore impact on work and family and other recovery issues. There may be a place for CBT for depression, anxiety management and understanding personality style. Examination of issues and working on self-management strategies are important in preventing future depression, improving resilience and maximising the individual’s psychological wellbeing.
Down Syndrome

DEFINITION
Source: http://www.merriam-webster.com/dictionary/Down%20syndrome
A congenital condition characterized by moderate to severe mental retardation, slanting eyes, a broad short skull, broad hands with short fingers, and trisomy of the human chromosome numbered 21.
SIGNS AND SYMPTOMS
Source: https://www.nichd.nih.gov/health/topics/down/conditioninfo/Pages/symptoms.aspx
Physical Symptoms
Common physical signs of Down syndrome include:
Intellectual and Developmental Symptoms
Cognitive impairment, problems with thinking and learning, is common in people with Down syndrome and usually ranges from mild to moderate. Only rarely is Down syndrome associated with severe cognitive impairment.
Other common cognitive and behavioral problems may include:
CAUSES
Source: http://www.healthcommunities.com/down-syndrome/children/causes-risk-factors-for-down-syndrome.shtml
Down syndrome results from cell division errors, either prior to or at conception. Trisomy 21 is caused by nondisjunction during cell division (condition in which a pair of chromosomes does not properly separate).
Normally, all cells have 23 pairs of matching chromosomes, 46 chromosomes in all. When egg and sperm cells divide in two, they distribute their 46 chromosomes equally—one chromosome from each pair moves to one of the resulting cells, forming two cells with 23 single chromosomes each. At fertilization, the resulting embryo receives 23 chromosomes each from the egg and sperm cells, bringing the total to 46 (23 pairs).
When nondisjunction occurs, chromosome 21 is not equally distributed when the egg or sperm cell divides, leaving one of the resulting cells with two copies of chromosome 21, instead of one. If this is the egg or sperm cell that gets fertilized, the abnormal cell contributes two copies of chromosome 21 to the embryo, which then has three copies (also including one copy from the normal egg or sperm cell). As the embryo grows, the extra copy becomes part of every cell thereafter.
Mosaic Down syndrome develops in a similar way, but nondisjunction occurs after fertilization, when the embryo is undergoing its own first series of cell divisions. This is why a person with mosaic Down syndrome has the correct number of chromosomes in some cells and the extra chromosome 21 in others.
Translocation Down syndrome is caused by abnormal cell division as well. In this case, when the cell divides, a piece of chromosome 21 breaks off and attaches itself to another chromosome. Even though the resulting cells have the correct number of chromosomes, the extra genetic material from chromosome 21 causes symptoms of Down syndrome.
Medical professionals know Down syndrome occurs because of the duplicated genetic material from chromosome 21, but they do not know why abnormal cell divisions occur.
RISK FACTORS
DIAGNOSIS
Source : http://www.healthcommunities.com/down-syndrome/children/diagnosis-of-down-syndrome.shtml
In most cases, Down syndrome is diagnosed at birth. Diagnosis involves a physical examination and diagnostic tests (e.g., blood tests). Signs of Down syndrome that are related to the baby's appearance often are apparent at birth. If a newborn exhibits signs of the condition (e.g., flat face, eyes that slant upward unrelated to ethnicity, ears that fold at the top), additional testing is performed to confirm the diagnosis.
Diagnostic tests for Down syndrome include a test called the chromosome karyotype test, which uses cells from a blood sample. By photographing the newborn's blood cells, physicians can group and organize the chromosomes to accurately determine whether an extra chromosome 21 is present.
Prenatal Tests for Down Syndrome
A number of prenatal tests are available to help pregnant women learn more about their risk for having a baby with Down syndrome. During pregnancy, screening tests provide a general idea of the risk and diagnostic tests can determine with 98–99 percent accuracy whether the unborn baby has the condition. Because they carry a small risk for miscarriage, diagnostic tests are conducted only when preliminary screening tests show cause for concern.
The maternal serum screening test is a blood test that generally is offered to women, usually between the 15th and 20th week of pregnancy. In this test, physicians look for abnormal levels of pregnancy-associated plasma protein (PAPP-A) and the hormones estriol and human chorionic gonadotropin (HCG). If any of these substances are higher than normal, there may be an increased risk that the unborn baby has Down syndrome. However, this test is only 60 percent accurate.
The maternal serum screening test may be performed with an ultrasound (sonogram) screening, which uses high frequency sound waves to create images that allow physicians to look for "markers" related to Down syndrome. Many doctors recommend both screening tests as a two-step process, taking the mother's age into account.
One type of ultrasound screening, the nuchal translucency screening test analyzes the area behind the unborn baby's neck. Babies with Down syndrome or with other chromosomal disorders tend to have more fluid in this area, making the space appear larger on ultrasound. Overall, this test is about 80 percent accurate.
A quad marker screen test is also available. This maternal blood test can be used to check for a number of birth defects, genetic conditions, and chromosomal disorders, including Down syndrome and spina bifida.
Three types of prenatal diagnostic tests are available. These tests are more conclusive than prenatal screening tests.
Amniocentesis is performed between 15 and 22 weeks of pregnancy. In this test, physicians use a needle to take a sample of the amniotic fluid around the fetus. The sample is then checked for chromosomal abnormalities. The risk for miscarriage caused by amniocentesis is 1 in 200.
Chorionic villus sampling (CVS) can be performed between 9 and 14 weeks. In this procedure, a sample of the placenta is removed and used to analyze the fetus’s chromosomes. The risk for miscarriage from CVS is 1 in 100 (about 1 percent).
Percutaneous umbilical blood sampling (PUBS) is conducted after 18 weeks of pregnancy. In this test, doctors remove a blood sample from a vein in the umbilical cord and use the sample to analyze the unborn baby's chromosomes. This test carries a higher risk for miscarriage (about 2%) than amniocentesis or CVS, so it is only performed when it is thought to be absolutely necessary.
TREATMENT
Source: https://www.nichd.nih.gov/health/topics/down/conditioninfo/pages/treatments.aspx
What are common treatments for Down syndrome?
There is no single, standard treatment for Down syndrome. Treatments are based on each individual's physical and intellectual needs as well as his or her personal strengths and limitations.1 People with Down syndrome can receive proper care while living at home and in the community.
A child with Down syndrome likely will receive care from a team of health professionals, including, but not limited to, physicians, special educators, speech therapists, occupational therapists, physical therapists, and social workers. All professionals who interact with children with Down syndrome should provide stimulation and encouragement.
People with Down syndrome are at a greater risk for a number of health problems and conditions than are those who do not have Down syndrome. Many of these associated conditions may require immediate care right after birth, occasional treatment throughout childhood and adolescence, or long-term treatments throughout life. For example, an infant with Down syndrome may need surgery a few days after birth to correct a heart defect; or a person with Down syndrome may have digestive problems that require a lifelong special diet.
Early Intervention and Educational Therapy
“Early intervention” refers to a range of specialized programs and resources that professionals provide to very young children with Down syndrome and their families. These professionals may include special educators, speech therapists, occupational therapists, physical therapists, and social workers.
Research indicates that early intervention improves outcomes for children with Down syndrome.This assistance can begin shortly after birth and often continues until a child reaches age 3.After that age, most children receive interventions and treatment through their local school district.
Most children with Down syndrome are eligible for free, appropriate public education under federal law. Public Law 105-17 (2004): The Individuals with Disabilities Education Act (IDEA) makes it possible for children with disabilities to get free educational services and devices to help them learn as much as they can. Each child is entitled to these services from birth through the end of high school, or until age 21, whichever comes first. Most early intervention programs fall under this legislation.
The National Early Childhood Technical Assistance Center, run by the U.S. Department of Education, provides information and resources for parents and families looking for early intervention programs.
The law also states that each child must be taught in the least restrictive environment that is appropriate. This statement does not mean that each child will be placed in a regular classroom. Instead, educators will work to provide an environment that best fits the child's needs and skills.
The following information may be helpful for those considering educational assistance programs for a child with Down syndrome:
The child must have certain cognitive or learning deficits to be eligible for free special education programs. Parents can contact a local school principal or special education coordinator to learn how to have a child examined to see if he or she qualifies for services under the IDEA.
If a child qualifies for special services, a team of people will work together to design an Individualized Educational Plan (IEP) for the child. The team may include parents or caregivers, teachers, a school psychologist, and other specialists in child development or education. The IEP includes specific learning goals for that child, based on his or her needs and capabilities. The team also decides how best to carry out the IEP.
Children with Down syndrome may attend a school for children with special needs. Parents may have a choice between a school where most of the children do not have disabilities and one for children with special needs. Educators and health care providers can help families with the decision about what environment is best. Integration into a regular school has become much more common in recent decades, and IDEA requires that public schools work to maximize a child's access to typical learning experiences and interactions.5
The U.S. Department of Education funds the Parent Center Network, which provides resources, contacts, and assistance for parents and families trying to navigate special education programs. Visit http://www.parentcenternetwork.org/External Web Site Policy for more information.
Therapies
A variety of therapies can be used in early intervention programs and throughout a person's life to promote the greatest possible development, independence, and productivity. Some of these therapies are listed below.
Drugs and Supplements
Some people with Down syndrome take amino acid supplements or drugs that affect their brain activity. However, many of the recent clinical trials of these treatments were poorly controlled and revealed adverse effects from these treatments. Since then, newer psychoactive drugs that are much more specific have been developed. No controlled clinical studies of these medications for Down syndrome have demonstrated their safety and efficacy, however.
Many studies of drugs to treat symptoms of dementia in Down syndrome have included only a few participants. The results of these studies have not shown clear benefits of these drugs, either. Similarly, studies of antioxidants for dementia in Down syndrome have shown that these supplements are safe, but not effective.
Assistive Devices
More and more often, interventions for children with Down syndrome involve assistive devices—any type of material, equipment, tool, or technology that enhances learning or makes tasks easier to complete. Examples include amplification devices for hearing problems, bands that help with movement, special pencils to make writing easier, touchscreen computers, and computers with large-letter keyboards.
DS-Connect®: The Down Syndrome Registry
Parents and families of children with Down syndrome can connect with other families and people with Down syndrome from around the world to learn more and share information. The NICHD-led DS-Connect® is a safe and secure registry to help families and researchers identify similarities and differences in the symptoms and treatment of people with Down syndrome and guide future research.
Example Case 1
Source: http://www.katemeadsassociates.com/case-studies/item/downs-syndrome-adult
Background History
Jane is 21 years old and has Downs Syndrome. She lives with her mother, father, older brother and pet dog. Her father works full time and her mother remains at home to support Jane. Jane and her family recently moved to the area from the north of the country where she had previously engaged in many groups and hobbies. Her hobbies were dancing, drama and art. She also had a volunteering job at a local nursing home where she handed out the tea and coffee. Since moving house, Jane has no hobbies and spends all day with her mother watching television and DVD’s. Jane has good verbal communication and is independently mobile.
Reason For Referral
Jane was referred for occupational therapy by her GP having demonstrated regular difficulties with low mood and aggressive behaviour. She was regularly physically aggressive towards her parents and often tearful. Jane was unable to explain her behaviour and her relationship with her family was rapidly deteriorating as her behaviour worsened.
Occupational Therapy Assessment
Jane received a full physical health check by her GP which showed no apparent physical cause for her symptoms. Jane was receiving support from a nurse who was monitoring her medication and ensuring that she received regular health checks such as dentist and optician appointments. Since physical causes of Jane’s behaviour had been ruled out, occupational therapy embarked on a goal to identify the cause of her difficulties and to support her and her family in reducing them.
Jane was assessed by occupational therapy using a variety of standardised and non standardised tools. These included formal assessments such as the Model of Human Occupation Screening Tool (MOHOST) and the Assessment of Motor and Processing Skills (AMPS). These assessments were augmented with informal interviews with Jane’s family, an environmental assessment, observation of functional tasks and completion of an interests check list.
This assessment identified that:
Jane had difficulties with the sequencing of tasks, identifying which order to carry out tasks in; She also had difficulty with standing for long periods of time; Jane lacked motivation to complete domestic and self care tasks; An environmental assessment and observation identified a significant level of auditory (noise) and visual stimulus when Jane was expected to carry out a task - for example, the television would be on in the lounge, the microwave and radio on in the kitchen in addition to which her dog was a very vocal creature and regularly contributed to the noise levels; Jane’s difficulties resulted in her parents completing a lot of her activities of daily living as they believed that she was unable to do so. She was also fully supported with her personal care; Jane appeared to lack meaningful occupation in her day and it was hypothesised that the low mood and challenging behaviour were a result of this lack of occupation. She was likely to be feeling bored and frustrated and her self esteem was deteriorating.
Occupational Therapy Treatment Plan
Jane and her family received an occupational therapy programme consisting of 12 weekly sessions of between 1 and 1.5 hours' duration.
The sessions focused on:
Using visual sequences for personal care and simple meal preparation which enabled Jane to wash and dress with minimal support. She was also able to make her own breakfast and drinks; Enabling Jane to carry out more complex tasks in the kitchen by supplying her with a perching stool; Placing visual indicators on the washing machine settings enabling Jane to do her own laundry; Supporting the family to understand Jane’s difficulties with distractions and reducing auditory stimuli in the home; Supporting the family to help Jane be as independent as possible by only completing the specific part of the task that she struggled with rather than completing the whole task eg opening a tight jar lid rather than making the whole sandwich; Giving Jane her own chores in the home such as the family laundry and dusting which she was praised for doing. Jane also helped her mother make the evening meal at least twice a week; Supporting Jane to look into accessing appropriate volunteering opportunities in the area. Jane was also referred to social services with a view to having a personal assistant who could support her in accessing the community without her family. She was also supported to engage with the local gym and drama group.
Outcome
As a result of the occupational therapy input and collaborative working with other agencies:-
Jane’s challenging behaviour reduced significantly; Her mood improved as she began to engage more and access her local community regularly; There was a noticeable reduction in the amount of times she was seen crying; Her relationship with her family improved dramatically - Jane is now able to help her mother with daily tasks and is praised on a daily basis for this help. In addition Jane’s mother was able to enrol onto a local college course as she had more free time which improved her own mood and energy levels enabling them to spend quality time together when they were both free.
Jane achieved all the goals that were set in the original assessment. She gave verbal feedback that she enjoyed working with the occupational therapist and was sad that she was not going to see them anymore.
Source: http://www.merriam-webster.com/dictionary/Down%20syndrome
A congenital condition characterized by moderate to severe mental retardation, slanting eyes, a broad short skull, broad hands with short fingers, and trisomy of the human chromosome numbered 21.
SIGNS AND SYMPTOMS
Source: https://www.nichd.nih.gov/health/topics/down/conditioninfo/Pages/symptoms.aspx
Physical Symptoms
Common physical signs of Down syndrome include:
- Decreased or poor muscle tone
- Short neck, with excess skin at the back of the neck
- Flattened facial profile and nose
- Small head, ears, and mouth
- Upward slanting eyes, often with a skin fold that comes out from the upper eyelid and covers the inner corner of the eye
- White spots on the colored part of the eye (called Brushfield spots)
- Wide, short hands with short fingers
- A single, deep, crease across the palm of the hand
- A deep groove between the first and second toes
Intellectual and Developmental Symptoms
Cognitive impairment, problems with thinking and learning, is common in people with Down syndrome and usually ranges from mild to moderate. Only rarely is Down syndrome associated with severe cognitive impairment.
Other common cognitive and behavioral problems may include:
- Short attention span
- Poor judgment
- Impulsive behavior
- Slow learning
- Delayed language and speech development
CAUSES
Source: http://www.healthcommunities.com/down-syndrome/children/causes-risk-factors-for-down-syndrome.shtml
Down syndrome results from cell division errors, either prior to or at conception. Trisomy 21 is caused by nondisjunction during cell division (condition in which a pair of chromosomes does not properly separate).
Normally, all cells have 23 pairs of matching chromosomes, 46 chromosomes in all. When egg and sperm cells divide in two, they distribute their 46 chromosomes equally—one chromosome from each pair moves to one of the resulting cells, forming two cells with 23 single chromosomes each. At fertilization, the resulting embryo receives 23 chromosomes each from the egg and sperm cells, bringing the total to 46 (23 pairs).
When nondisjunction occurs, chromosome 21 is not equally distributed when the egg or sperm cell divides, leaving one of the resulting cells with two copies of chromosome 21, instead of one. If this is the egg or sperm cell that gets fertilized, the abnormal cell contributes two copies of chromosome 21 to the embryo, which then has three copies (also including one copy from the normal egg or sperm cell). As the embryo grows, the extra copy becomes part of every cell thereafter.
Mosaic Down syndrome develops in a similar way, but nondisjunction occurs after fertilization, when the embryo is undergoing its own first series of cell divisions. This is why a person with mosaic Down syndrome has the correct number of chromosomes in some cells and the extra chromosome 21 in others.
Translocation Down syndrome is caused by abnormal cell division as well. In this case, when the cell divides, a piece of chromosome 21 breaks off and attaches itself to another chromosome. Even though the resulting cells have the correct number of chromosomes, the extra genetic material from chromosome 21 causes symptoms of Down syndrome.
Medical professionals know Down syndrome occurs because of the duplicated genetic material from chromosome 21, but they do not know why abnormal cell divisions occur.
RISK FACTORS
- The age of the mother is an important consideration in assessing Down syndrome risk. As a woman gets older, her eggs are more likely to divide abnormally. At age 25, the risk for Down syndrome is 1 in 1,250 births. This risk increases to 1 in 385 at age 35 and jumps to 1 in 30 at age 45. However, 80 percent of babies with Down syndrome are born to mothers who are younger than age 35. The reason for this is that women under the age of 35 have a higher rate of giving birth.
- Women who have a child with Down syndrome are more likely to have another baby affected with the condition. Also, mothers who have Down syndrome themselves are 50 percent more likely to give birth to a child with Down syndrome.
- Parents can pass down a chromosomal abnormality called balanced translocation, which contributes to Translocation Down syndrome. In this instance, the parent does not have signs of Down syndrome, but has genetic material "balanced" between chromosome 21 and another chromosome, posing an increased risk for the child if that material attaches to the other chromosome when the cell divides. Not all cases of Translocation Down syndrome occur this way.
DIAGNOSIS
Source : http://www.healthcommunities.com/down-syndrome/children/diagnosis-of-down-syndrome.shtml
In most cases, Down syndrome is diagnosed at birth. Diagnosis involves a physical examination and diagnostic tests (e.g., blood tests). Signs of Down syndrome that are related to the baby's appearance often are apparent at birth. If a newborn exhibits signs of the condition (e.g., flat face, eyes that slant upward unrelated to ethnicity, ears that fold at the top), additional testing is performed to confirm the diagnosis.
Diagnostic tests for Down syndrome include a test called the chromosome karyotype test, which uses cells from a blood sample. By photographing the newborn's blood cells, physicians can group and organize the chromosomes to accurately determine whether an extra chromosome 21 is present.
Prenatal Tests for Down Syndrome
A number of prenatal tests are available to help pregnant women learn more about their risk for having a baby with Down syndrome. During pregnancy, screening tests provide a general idea of the risk and diagnostic tests can determine with 98–99 percent accuracy whether the unborn baby has the condition. Because they carry a small risk for miscarriage, diagnostic tests are conducted only when preliminary screening tests show cause for concern.
The maternal serum screening test is a blood test that generally is offered to women, usually between the 15th and 20th week of pregnancy. In this test, physicians look for abnormal levels of pregnancy-associated plasma protein (PAPP-A) and the hormones estriol and human chorionic gonadotropin (HCG). If any of these substances are higher than normal, there may be an increased risk that the unborn baby has Down syndrome. However, this test is only 60 percent accurate.
The maternal serum screening test may be performed with an ultrasound (sonogram) screening, which uses high frequency sound waves to create images that allow physicians to look for "markers" related to Down syndrome. Many doctors recommend both screening tests as a two-step process, taking the mother's age into account.
One type of ultrasound screening, the nuchal translucency screening test analyzes the area behind the unborn baby's neck. Babies with Down syndrome or with other chromosomal disorders tend to have more fluid in this area, making the space appear larger on ultrasound. Overall, this test is about 80 percent accurate.
A quad marker screen test is also available. This maternal blood test can be used to check for a number of birth defects, genetic conditions, and chromosomal disorders, including Down syndrome and spina bifida.
Three types of prenatal diagnostic tests are available. These tests are more conclusive than prenatal screening tests.
Amniocentesis is performed between 15 and 22 weeks of pregnancy. In this test, physicians use a needle to take a sample of the amniotic fluid around the fetus. The sample is then checked for chromosomal abnormalities. The risk for miscarriage caused by amniocentesis is 1 in 200.
Chorionic villus sampling (CVS) can be performed between 9 and 14 weeks. In this procedure, a sample of the placenta is removed and used to analyze the fetus’s chromosomes. The risk for miscarriage from CVS is 1 in 100 (about 1 percent).
Percutaneous umbilical blood sampling (PUBS) is conducted after 18 weeks of pregnancy. In this test, doctors remove a blood sample from a vein in the umbilical cord and use the sample to analyze the unborn baby's chromosomes. This test carries a higher risk for miscarriage (about 2%) than amniocentesis or CVS, so it is only performed when it is thought to be absolutely necessary.
TREATMENT
Source: https://www.nichd.nih.gov/health/topics/down/conditioninfo/pages/treatments.aspx
What are common treatments for Down syndrome?
There is no single, standard treatment for Down syndrome. Treatments are based on each individual's physical and intellectual needs as well as his or her personal strengths and limitations.1 People with Down syndrome can receive proper care while living at home and in the community.
A child with Down syndrome likely will receive care from a team of health professionals, including, but not limited to, physicians, special educators, speech therapists, occupational therapists, physical therapists, and social workers. All professionals who interact with children with Down syndrome should provide stimulation and encouragement.
People with Down syndrome are at a greater risk for a number of health problems and conditions than are those who do not have Down syndrome. Many of these associated conditions may require immediate care right after birth, occasional treatment throughout childhood and adolescence, or long-term treatments throughout life. For example, an infant with Down syndrome may need surgery a few days after birth to correct a heart defect; or a person with Down syndrome may have digestive problems that require a lifelong special diet.
Early Intervention and Educational Therapy
“Early intervention” refers to a range of specialized programs and resources that professionals provide to very young children with Down syndrome and their families. These professionals may include special educators, speech therapists, occupational therapists, physical therapists, and social workers.
Research indicates that early intervention improves outcomes for children with Down syndrome.This assistance can begin shortly after birth and often continues until a child reaches age 3.After that age, most children receive interventions and treatment through their local school district.
Most children with Down syndrome are eligible for free, appropriate public education under federal law. Public Law 105-17 (2004): The Individuals with Disabilities Education Act (IDEA) makes it possible for children with disabilities to get free educational services and devices to help them learn as much as they can. Each child is entitled to these services from birth through the end of high school, or until age 21, whichever comes first. Most early intervention programs fall under this legislation.
The National Early Childhood Technical Assistance Center, run by the U.S. Department of Education, provides information and resources for parents and families looking for early intervention programs.
The law also states that each child must be taught in the least restrictive environment that is appropriate. This statement does not mean that each child will be placed in a regular classroom. Instead, educators will work to provide an environment that best fits the child's needs and skills.
The following information may be helpful for those considering educational assistance programs for a child with Down syndrome:
The child must have certain cognitive or learning deficits to be eligible for free special education programs. Parents can contact a local school principal or special education coordinator to learn how to have a child examined to see if he or she qualifies for services under the IDEA.
If a child qualifies for special services, a team of people will work together to design an Individualized Educational Plan (IEP) for the child. The team may include parents or caregivers, teachers, a school psychologist, and other specialists in child development or education. The IEP includes specific learning goals for that child, based on his or her needs and capabilities. The team also decides how best to carry out the IEP.
Children with Down syndrome may attend a school for children with special needs. Parents may have a choice between a school where most of the children do not have disabilities and one for children with special needs. Educators and health care providers can help families with the decision about what environment is best. Integration into a regular school has become much more common in recent decades, and IDEA requires that public schools work to maximize a child's access to typical learning experiences and interactions.5
The U.S. Department of Education funds the Parent Center Network, which provides resources, contacts, and assistance for parents and families trying to navigate special education programs. Visit http://www.parentcenternetwork.org/External Web Site Policy for more information.
Therapies
A variety of therapies can be used in early intervention programs and throughout a person's life to promote the greatest possible development, independence, and productivity. Some of these therapies are listed below.
- Physical therapy includes activities and exercises that help build motor skills, increase muscle strength, and improve posture and balance.
- Physical therapy is important, especially early in a child's life, because physical abilities lay the foundation for other skills. The ability to turn over, crawl, and reach helps infants learn about the world around them and how to interact with it.
- A physical therapist also can help a child with Down syndrome compensate for physical challenges, such as low muscle tone, in ways that avoid long-term problems. For example, a physical therapist might help a child establish an efficient walking pattern, rather than one that might lead to foot pain.
- Speech-language therapy can help children with Down syndrome improve their communication skills and use language more effectively.
- Children with Down syndrome often learn to speak later than their peers. A speech-language therapist can help them develop the early skills necessary for communication, such as imitating sounds. The therapist also may help an infant breastfeed because breastfeeding can strengthen muscles that are used for speech.
- In many cases, children with Down syndrome understand language and want to communicate before they can speak. A speech-language therapist can help a child use alternate means of communication, such as sign language and pictures, until he or she learns to speak.
- Learning to communicate is an ongoing process, so a person with Down syndrome also may benefit from speech and language therapy in school as well as later in life. The therapist may help with conversation skills, pronunciation skills, understanding what is read (called comprehension), and learning and remembering words.
- Occupational therapy helps find ways to adjust everyday tasks and conditions to match a person's needs and abilities.
- This type of therapy teaches self-care skills such as eating, getting dressed, writing, and using a computer.
- An occupational therapist might offer special tools that can help improve everyday functioning, such as a pencil that is easier to grip.
- At the high school level, an occupational therapist could help teenagers identify jobs, careers, or skills that match their interests and strengths.
- Emotional and behavioral therapies work to find useful responses to both desirable and undesirable behaviors. Children with Down syndrome may become frustrated because of difficulty communicating, may develop compulsive behaviors, and may have Attention Deficit Hyperactivity Disorder and other mental health issues. These types of therapists try to understand why a child is acting out, create ways and strategies for avoiding or preventing these situations from occurring, and teach better or more positive ways to respond to situations.
- A psychologist, counselor, or other mental health professional can help a child deal with emotions and build coping and interpersonal skills.
- The changes in hormone levels that adolescents experience during puberty can cause them to become more aggressive. Behavioral therapists can help teenagers recognize their intense emotions and teach them healthy ways to reach a feeling of calmness.
- Parents may also benefit from guidance on how to help a child with Down syndrome manage day-to-day challenges and reach his or her full potential.
Drugs and Supplements
Some people with Down syndrome take amino acid supplements or drugs that affect their brain activity. However, many of the recent clinical trials of these treatments were poorly controlled and revealed adverse effects from these treatments. Since then, newer psychoactive drugs that are much more specific have been developed. No controlled clinical studies of these medications for Down syndrome have demonstrated their safety and efficacy, however.
Many studies of drugs to treat symptoms of dementia in Down syndrome have included only a few participants. The results of these studies have not shown clear benefits of these drugs, either. Similarly, studies of antioxidants for dementia in Down syndrome have shown that these supplements are safe, but not effective.
Assistive Devices
More and more often, interventions for children with Down syndrome involve assistive devices—any type of material, equipment, tool, or technology that enhances learning or makes tasks easier to complete. Examples include amplification devices for hearing problems, bands that help with movement, special pencils to make writing easier, touchscreen computers, and computers with large-letter keyboards.
DS-Connect®: The Down Syndrome Registry
Parents and families of children with Down syndrome can connect with other families and people with Down syndrome from around the world to learn more and share information. The NICHD-led DS-Connect® is a safe and secure registry to help families and researchers identify similarities and differences in the symptoms and treatment of people with Down syndrome and guide future research.
Example Case 1
Source: http://www.katemeadsassociates.com/case-studies/item/downs-syndrome-adult
Background History
Jane is 21 years old and has Downs Syndrome. She lives with her mother, father, older brother and pet dog. Her father works full time and her mother remains at home to support Jane. Jane and her family recently moved to the area from the north of the country where she had previously engaged in many groups and hobbies. Her hobbies were dancing, drama and art. She also had a volunteering job at a local nursing home where she handed out the tea and coffee. Since moving house, Jane has no hobbies and spends all day with her mother watching television and DVD’s. Jane has good verbal communication and is independently mobile.
Reason For Referral
Jane was referred for occupational therapy by her GP having demonstrated regular difficulties with low mood and aggressive behaviour. She was regularly physically aggressive towards her parents and often tearful. Jane was unable to explain her behaviour and her relationship with her family was rapidly deteriorating as her behaviour worsened.
Occupational Therapy Assessment
Jane received a full physical health check by her GP which showed no apparent physical cause for her symptoms. Jane was receiving support from a nurse who was monitoring her medication and ensuring that she received regular health checks such as dentist and optician appointments. Since physical causes of Jane’s behaviour had been ruled out, occupational therapy embarked on a goal to identify the cause of her difficulties and to support her and her family in reducing them.
Jane was assessed by occupational therapy using a variety of standardised and non standardised tools. These included formal assessments such as the Model of Human Occupation Screening Tool (MOHOST) and the Assessment of Motor and Processing Skills (AMPS). These assessments were augmented with informal interviews with Jane’s family, an environmental assessment, observation of functional tasks and completion of an interests check list.
This assessment identified that:
Jane had difficulties with the sequencing of tasks, identifying which order to carry out tasks in; She also had difficulty with standing for long periods of time; Jane lacked motivation to complete domestic and self care tasks; An environmental assessment and observation identified a significant level of auditory (noise) and visual stimulus when Jane was expected to carry out a task - for example, the television would be on in the lounge, the microwave and radio on in the kitchen in addition to which her dog was a very vocal creature and regularly contributed to the noise levels; Jane’s difficulties resulted in her parents completing a lot of her activities of daily living as they believed that she was unable to do so. She was also fully supported with her personal care; Jane appeared to lack meaningful occupation in her day and it was hypothesised that the low mood and challenging behaviour were a result of this lack of occupation. She was likely to be feeling bored and frustrated and her self esteem was deteriorating.
Occupational Therapy Treatment Plan
Jane and her family received an occupational therapy programme consisting of 12 weekly sessions of between 1 and 1.5 hours' duration.
The sessions focused on:
Using visual sequences for personal care and simple meal preparation which enabled Jane to wash and dress with minimal support. She was also able to make her own breakfast and drinks; Enabling Jane to carry out more complex tasks in the kitchen by supplying her with a perching stool; Placing visual indicators on the washing machine settings enabling Jane to do her own laundry; Supporting the family to understand Jane’s difficulties with distractions and reducing auditory stimuli in the home; Supporting the family to help Jane be as independent as possible by only completing the specific part of the task that she struggled with rather than completing the whole task eg opening a tight jar lid rather than making the whole sandwich; Giving Jane her own chores in the home such as the family laundry and dusting which she was praised for doing. Jane also helped her mother make the evening meal at least twice a week; Supporting Jane to look into accessing appropriate volunteering opportunities in the area. Jane was also referred to social services with a view to having a personal assistant who could support her in accessing the community without her family. She was also supported to engage with the local gym and drama group.
Outcome
As a result of the occupational therapy input and collaborative working with other agencies:-
Jane’s challenging behaviour reduced significantly; Her mood improved as she began to engage more and access her local community regularly; There was a noticeable reduction in the amount of times she was seen crying; Her relationship with her family improved dramatically - Jane is now able to help her mother with daily tasks and is praised on a daily basis for this help. In addition Jane’s mother was able to enrol onto a local college course as she had more free time which improved her own mood and energy levels enabling them to spend quality time together when they were both free.
Jane achieved all the goals that were set in the original assessment. She gave verbal feedback that she enjoyed working with the occupational therapist and was sad that she was not going to see them anymore.
BRAIN TUMORS

DEFINITION
Source: http://www.healthline.com/health/brain-tumor#Overview1
SIGNS AND SYMPTOMS
Source: http://www.healthline.com/health/brain-tumor#Symptoms4
Headaches are a common symptom of a brain tumor. You may experience headaches that:
The following symptoms can occur with pituitary tumors:
CAUSES
Source: http://www.mayoclinic.org/diseases-conditions/brain-tumor/symptoms-causes/dxc-20117134
Brain tumors that begin in the brain
Many different types of primary brain tumors exist. Each gets its name from the type of cells involved. Examples include:
Cancer that begins elsewhere and spreads to the brain
Any cancer can spread to the brain, but the most common types include:
RISK FACTORS
Risk factors for brain tumors include:
Source: http://www.healthline.com/health/brain-tumor#RiskFactors3
Family History
DIAGNOSIS
Source: http://www.healthline.com/health/brain-tumor#Diagnosis5
Diagnosis of a brain tumor begins with a physical exam and a look at your medical history.
The physical exam includes a very detailed neurological examination. Your doctor will conduct a test to see if your cranial nerves are intact. These are the nerves that originate in your brain.
Your doctor will look inside your eyes with an ophthalmoscope, which is an instrument that shines a light through your pupils and onto your retinas. This allows your doctor to check how your pupils react to light. It also allows your doctor to look directly into your eyes to see if there’s any swelling of the optic nerve. When pressure increases inside the skull, changes in the optic nerve can occur.
The doctor may also evaluate your:
CT Scan of the Head
TREATMENT
Source: http://www.healthline.com/health/brain-tumor#Treatment6
The treatment of a brain tumor depends on:
Risks of brain surgery include infection and bleeding. Clinically dangerous benign tumors are also surgically removed. Metastatic brain tumors are treated according to guidelines for the type of original cancer.
Surgery can be combined with other treatments, such as radiation therapy and chemotherapy.
Physical therapy, occupational therapy, and speech therapy can help you to recover after neurosurgery.
Extra Information
Source: http://abc2.org/guidance/brain-cancer-facts/tumor-grades-and-types?gclid=CLC6lseJ48wCFQVwvAodV0UMLg
Tumor Grades and Types
When most normal cells grow old or get damaged, they die, and new cells take their place. Sometimes, this process goes wrong. New cells form when the body doesn't need them, and old or damaged cells don't die as they should. The buildup of extra cells often forms a mass of tissue called a growth or tumor. Primary brain tumors can be benign or malignant.Benign brain tumors do not contain cancer cells. Usually, benign tumors can be removed, and they seldom grow back.Benign brain tumors usually have an obvious border or edge. Cells from benign tumors rarely invade tissues around them. They don't spread to other parts of the body. However, benign tumors can press on sensitive areas of the brain and cause serious health problems. Unlike benign tumors in most other parts of the body, benign brain tumors are sometimes life threatening. Benign brain tumors may become malignant. Malignant brain tumors (also called brain cancer) contain cancer cells: Malignant brain tumors are generally more serious and often are a threat to life. They are likely to grow rapidly and crowd or invade the nearby healthy brain tissue. Cancer cells may break away from malignant brain tumors and spread to other parts of the brain or to the spinal cord. They rarely spread to other parts of the body.
Related: 10 Steps for Managing a Brain Tumor Diagnosis
Tumor Grade
Doctors group brain tumors by grade. The grade of a tumor refers to the way the cells look under a microscope:
Over time, a low-grade tumor may become a high-grade tumor. However, the change to a high-grade tumor happens more often among adults than children.
Types of Primary Brain Tumors
There are many types of primary brain tumors. Primary brain tumors are named according to the type of cells or the part of the brain in which they begin. For example, most primary brain tumors begin in glial cells. This type of tumor is called a glioma.
Among adults, the most common types are:
Among children, the most common types are:
Source: http://www.healthline.com/health/brain-tumor#Overview1
- A brain tumor is a collection, or mass, of abnormal cells in your brain. Your skull, which encloses your brain, is very rigid. Any growth inside such a restricted space can cause problems. Brain tumors can be cancerous or non-cancerous. When benign or malignant tumors grow, they can cause the pressure inside your skull to increase. This can cause brain damage, and it can be life-threatening.
- Brain tumors are categorized as primary or secondary. A primary brain tumor originates in your brain. Many primary brain tumors are benign. A secondary brain tumor, also known as a metastatic brain tumor, occurs when cancer cells spread to your brain from another organ, such as your lung or breast.
SIGNS AND SYMPTOMS
Source: http://www.healthline.com/health/brain-tumor#Symptoms4
- Symptoms of brain tumors depend on the location and size of the tumor. Tumors cause direct damage by invading brain tissue and causing brain pressure to increase. You’ll have noticeable symptoms when a growing tumor is putting pressure on your brain tissue.
Headaches are a common symptom of a brain tumor. You may experience headaches that:
- are worse in the morning when waking up
- occur while you’re sleeping
- are made worse by coughing, sneezing, or exercise
- vomiting
- blurred vision or double vision
- confusion
- seizures (especially in adults)
- weakness of a limb or part of the face
- a change in mental functioning
- Other common symptoms include:
- clumsiness
- memory loss
- confusion
- difficulty writing or reading
- changes in the ability to hear, taste, or smell
- decreased alertness, which may include drowsiness and loss of consciousness
- difficulty swallowing
- dizziness or vertigo
- eye problems, such as drooping eyelids and unequal pupils
- uncontrollable movements
- hand tremors
- loss of balance
- loss of bladder or bowel control
- numbness or tingling on one side of the body
- trouble speaking or understanding what others are saying
- changes in mood, personality, emotions, and behavior
- difficulty walking
- muscle weakness in the face, arm, or leg
- Symptoms of Pituitary Tumors
The following symptoms can occur with pituitary tumors:
- nipple discharge, or galactorrhea
- lack of menstruation in women
- development of breast tissue in men, or gynecomastia
- enlargement of the hands and feet
- sensitivity to heat or cold
- increased amounts of body hair, or hirsutism
- low blood pressure
- obesity
CAUSES
Source: http://www.mayoclinic.org/diseases-conditions/brain-tumor/symptoms-causes/dxc-20117134
Brain tumors that begin in the brain
- Primary brain tumors originate in the brain itself or in tissues close to it, such as in the brain-covering membranes (meninges), cranial nerves, pituitary gland or pineal gland.
- Primary brain tumors begin when normal cells acquire errors (mutations) in their DNA. These mutations allow cells to grow and divide at increased rates and to continue living when healthy cells would die. The result is a mass of abnormal cells, which forms a tumor.
- Primary brain tumors are much less common than are secondary brain tumors, in which cancer begins elsewhere and spreads to the brain.
Many different types of primary brain tumors exist. Each gets its name from the type of cells involved. Examples include:
- Gliomas. These tumors begin in the brain or spinal cord and include astrocytomas, ependymoma, glioblastomas, oligoastrocytomas and oligodendrogliomas.
- Meningiomas. A meningioma is a tumor that arises from the membranes that surround your brain and spinal cord (meninges). Most meningiomas are noncancerous.
- Acoustic neuromas (schwannomas). These are benign tumors that develop on the nerves that control balance and hearing leading from your inner ear to your brain.
- Pituitary adenomas. These are mostly benign tumors that develop in the pituitary gland at the base of the brain. These tumors can affect the pituitary hormones with effects throughout the body.
- Medulloblastomas. These are the most common cancerous brain tumors in children. A medulloblastoma starts in the lower back part of the brain and tends to spread through the spinal fluid. These tumors are less common in adults, but they do occur.
- PNETs. Primitive neuroectodermal tumors (PNETs) are rare, cancerous tumors that start in embryonic (fetal) cells in the brain. They can occur anywhere in the brain.
- Germ cell tumors. Germ cell tumors may develop during childhood where the testicles or ovaries will form. But sometimes germ cell tumors move to other parts of the body, such as the brain.
- Craniopharyngiomas. These rare, noncancerous tumors start near the brain's pituitary gland, which secretes hormones that control many body functions. As the craniopharyngioma slowly grows, it can affect the pituitary gland and other structures near the brain.
Cancer that begins elsewhere and spreads to the brain
- Secondary (metastatic) brain tumors are tumors that result from cancer that starts elsewhere in your body and then spreads (metastasizes) to your brain.
- Secondary brain tumors most often occur in people who have a history of cancer. But in rare cases, a metastatic brain tumor may be the first sign of cancer that began elsewhere in your body.
- Secondary brain tumors are far more common than are primary brain tumors.
Any cancer can spread to the brain, but the most common types include:
- Breast cancer
- Colon cancer
- Kidney cancer
- Lung cancer
- Melanoma
RISK FACTORS
Risk factors for brain tumors include:
Source: http://www.healthline.com/health/brain-tumor#RiskFactors3
Family History
- Only about 5 to 10 percent of all cancers are genetically inherited, or hereditary. It’s rare for a brain tumor to be genetically inherited. Talk to your doctor if several people in your family have been diagnosed with a brain tumor. Your doctor can recommend a genetic counselor for you.
- Risk for most types of brain tumors increases with age.
- Brain tumors are most likely to occur in Caucasians. However, African-American people are more likely to get meningiomas.
- Being exposed to certain chemicals, such as those you might find in a work environment, can increase your risk for brain cancer. The National Institute for Occupational Safety and Health keeps a list of potential cancer-causing chemicals found in work places.
- Exposure to Radiation
- People who have been exposed to ionizing radiation have an increased risk of brain tumors. You can be exposed to ionizing radiation through high-radiation cancer therapies. You can also be exposed to radiation from nuclear fallout. The nuclear power plant incidents in Fukushima and Chernobyl are examples of how people can be exposed to ionizing radiation.
- No History of Chicken Pox
- According to the American Brain Tumor Association, people with a history of childhood chicken pox have a decreased risk of getting brain tumors.
DIAGNOSIS
Source: http://www.healthline.com/health/brain-tumor#Diagnosis5
Diagnosis of a brain tumor begins with a physical exam and a look at your medical history.
The physical exam includes a very detailed neurological examination. Your doctor will conduct a test to see if your cranial nerves are intact. These are the nerves that originate in your brain.
Your doctor will look inside your eyes with an ophthalmoscope, which is an instrument that shines a light through your pupils and onto your retinas. This allows your doctor to check how your pupils react to light. It also allows your doctor to look directly into your eyes to see if there’s any swelling of the optic nerve. When pressure increases inside the skull, changes in the optic nerve can occur.
The doctor may also evaluate your:
- muscle strength
- coordination
- memory
- ability to do mathematical calculations
CT Scan of the Head
- CT scans are ways for your doctor get a more detailed scan of your body than they could with an X-ray machine. This can be done with or without contrast.
- Contrast is achieved in a CT scan of the head by using a special dye that helps doctors see some structures, like blood vessels, more clearly. You often have to fast before a CT scan that’s using contrast.
- If you have an MRI of your head, a special dye can be used to help your doctor detect tumors. An MRI is different from a CT scan because it doesn’t use radiation.
- This study uses a dye that’s injected into your artery, usually in the groin area. The dye travels to the arteries in your brain. It allows your doctor to see what the blood supply of the tumors looks like. This information is useful at the time of surgery.
- A brain scan uses harmless radioactive dye that’s injected into a vein. When the dye goes through the veins in the tumor, an image is taken.
- Brain tumors can cause breaks or fractures in the bones of the skull, and specific X-rays can show if this has occurred. These X-rays can also pick up calcium deposits, which are sometimes contained within a tumor. Calcium deposits may be in your bloodstream if your cancer has moved to your bones.
- A small piece of the tumor is obtained during a biopsy. A specialist called a neuropathologist will examine it. The biopsy will identify if the tumor cells are benign or malignant. It will also determine whether the cancer originated in your brain or another part of your body.
TREATMENT
Source: http://www.healthline.com/health/brain-tumor#Treatment6
The treatment of a brain tumor depends on:
- the type of tumor
- the size of the tumor
- the location of the tumor
- your general health
Risks of brain surgery include infection and bleeding. Clinically dangerous benign tumors are also surgically removed. Metastatic brain tumors are treated according to guidelines for the type of original cancer.
Surgery can be combined with other treatments, such as radiation therapy and chemotherapy.
Physical therapy, occupational therapy, and speech therapy can help you to recover after neurosurgery.
Extra Information
Source: http://abc2.org/guidance/brain-cancer-facts/tumor-grades-and-types?gclid=CLC6lseJ48wCFQVwvAodV0UMLg
Tumor Grades and Types
When most normal cells grow old or get damaged, they die, and new cells take their place. Sometimes, this process goes wrong. New cells form when the body doesn't need them, and old or damaged cells don't die as they should. The buildup of extra cells often forms a mass of tissue called a growth or tumor. Primary brain tumors can be benign or malignant.Benign brain tumors do not contain cancer cells. Usually, benign tumors can be removed, and they seldom grow back.Benign brain tumors usually have an obvious border or edge. Cells from benign tumors rarely invade tissues around them. They don't spread to other parts of the body. However, benign tumors can press on sensitive areas of the brain and cause serious health problems. Unlike benign tumors in most other parts of the body, benign brain tumors are sometimes life threatening. Benign brain tumors may become malignant. Malignant brain tumors (also called brain cancer) contain cancer cells: Malignant brain tumors are generally more serious and often are a threat to life. They are likely to grow rapidly and crowd or invade the nearby healthy brain tissue. Cancer cells may break away from malignant brain tumors and spread to other parts of the brain or to the spinal cord. They rarely spread to other parts of the body.
Related: 10 Steps for Managing a Brain Tumor Diagnosis
Tumor Grade
Doctors group brain tumors by grade. The grade of a tumor refers to the way the cells look under a microscope:
- Grade I: The tissue is benign. The cells look nearly like normal brain cells, and they grow slowly.
- Grade II: The tissue is malignant. The cells look less like normal cells than do the cells in a Grade I tumor.
- Grade III: The malignant tissue has cells that look very different from normal cells. The abnormal cells are actively growing (anaplastic).
- Grade IV: The malignant tissue has cells that look most abnormal and tend to grow quickly.
Over time, a low-grade tumor may become a high-grade tumor. However, the change to a high-grade tumor happens more often among adults than children.
Types of Primary Brain Tumors
There are many types of primary brain tumors. Primary brain tumors are named according to the type of cells or the part of the brain in which they begin. For example, most primary brain tumors begin in glial cells. This type of tumor is called a glioma.
Among adults, the most common types are:
- Astrocytoma: The tumor arises from star-shaped glial cells called astrocytes. It can be any grade. In adults, an astrocytoma most often arises in the cerebrum.
- Grade I or II astrocytoma: It may be called a low-grade glioma.
- Grade III astrocytoma: It's sometimes called a high-grade or an anaplastic astrocytoma.
- Grade IV astrocytoma: It may be called a glioblastoma or malignant astrocytic glioma.
- Meningioma: The tumor arises in the meninges. It can be grade I, II, or III. It's usually benign (grade I) and grows slowly.
- Oligodendroglioma: The tumor arises from cells that make the fatty substance that covers and protects nerves. It usually occurs in the cerebrum. It's most common in middle-aged adults. It can be grade II or III.
Among children, the most common types are:
- Medulloblastoma: The tumor usually arises in the cerebellum. It's sometimes called a primitive neuroectodermal tumor. It is grade IV.
- Grade I or II astrocytoma: In children, this low-grade tumor occurs anywhere in the brain. The most common astrocytoma among children is juvenile pilocytic astrocytoma. It's grade I.
- Ependymoma: The tumor arises from cells that line the ventricles or the central canal of the spinal cord. It's most commonly found in children and young adults. It can be grade I, II, or III.
- Brainstem glioma: The tumor occurs in the lowest part of the brain. It can be a low-grade or high-grade tumor. The most common type is diffuse intrinsic pontine glioma.
AUTISM
DEFINITION
Source: http://www.merriam-webster.com/dictionary/autism
A variable developmental disorder that appears by age three and is characterized by impairment of the ability to form normal social relationships, by impairment of the ability to communicate with others, and by stereotyped behavior patterns.
SIGNS AND SYMPTOMS
Source: https://www.autismspeaks.org/what-autism/symptoms
Autism spectrum disorders (ASD) are characterized by social-interaction difficulties, communication challenges and a tendency to engage in repetitive behaviors. However, symptoms and their severity vary widely across these three core areas. Taken together, they may result in relatively mild challenges for someone on the high functioning end of the autism spectrum. For others, symptoms may be more severe, as when repetitive behaviors and lack of spoken language interfere with everyday life. As illustrated by the graph above, the basic symptoms of autism are often accompanied other medical conditions and challenges. These, too, can vary widely in severity. While autism is usually a life-long condition, all children and adults benefit from interventions, or therapies, that can reduce symptoms and increase skills and abilities. Although it is best to begin intervention as soon as possible, the benefits of therapy can continue throughout life.
Social Challenges
Typically developing infants are social by nature. They gaze at faces, turn toward voices, grasp a finger and even smile by 2 to 3 months of age. By contrast, most children who develop autism have difficulty engaging in the give-and-take of everyday human interactions. By 8 to 10 months of age, many infants who go on to develop autism are showing some symptoms such as failure to respond to their names, reduced interest in people and delayed babbling. By toddlerhood, many children with autism have difficulty playing social games, don’t imitate the actions of others and prefer to play alone. They may fail to seek comfort or respond to parents' displays of anger or affection in typical ways.
Research suggests that children with autism are attached to their parents. However the way they express this attachment can be unusual. To parents, it may seem as if their child is disconnected. Both children and adults with autism also tend to have difficulty interpreting what others are thinking and feeling. Subtle social cures such as a smile, wave or grimace may convey little meaning. To a person who misses these social cues, a statement like “Come here!” may mean the same thing, regardless of whether the speaker is smiling and extending her arms for a hug or frowning and planting her fists on her hips. Without the ability to interpret gestures and facial expressions, the social world can seem bewildering.
Many persons with autism have similar difficulty seeing things from another person's perspective. Most five year olds understand that other people have different thoughts, feelings and goals than they have. A person with autism may lack such understanding. This, in turn, can interfere with the ability to predict or understand another person’s actions.
It is common – but not universal – for those with autism to have difficulty regulating emotions. This can take the form of seemingly “immature” behavior such as crying or having outbursts in inappropriate situations. It can also lead to disruptive and physically aggressive behavior. The tendency to “lose control” may be particularly pronounced in unfamiliar, overwhelming or frustrating situations. Frustration can also result in self-injurious behaviors such as head banging, hair pulling or self-biting.
Communication Difficulties
By age three, most children have passed predictable milestones on the path to learning language. One of the earliest is babbling. By the first birthday, most typically developing toddlers say a word or two, turn and look when they hear their names, point to objects they want or want to show to someone (not all cultures use pointing in this way). When offered something distasteful, they can make clear – by sound or expression – that the answer is “no.”
By contrast, young children with autism tend to be delayed in babbling and speaking and learning to use gestures. Some infants who later develop autism coo and babble during the first few months of life before losing these communicative behaviors. Others experience significant language delays and don’t begin to speak until much later. With therapy, however, most people with autism do learn to use spoken language and all can learn to communicate.
Many nonverbal or nearly nonverbal children and adults learn to use communication systems such as sign language, electronic word processors or even speech-generating devices.
When language begins to develop, the person with autism may use speech in unusual ways. Some have difficulty combining words into meaningful sentences. They may speak only single words or repeat the same phrase over and over. Some go through a stage where they repeat what they hear verbatim (echolalia).
Some mildly affected children exhibit only slight delays in language or even develop precocious language and unusually large vocabularies – yet have difficulty sustaining a conversation. Some children and adults with autism tend to carry on monologues on a favorite subject, giving others little chance to comment. In other words, the ordinary “give and take” of conversation proves difficult. Some children with ASD with superior language skills tend to speak like little professors, failing to pick up on the “kid-speak” that’s common among their peers.
Another common difficulty is the inability to understand body language, tone of voice and expressions that aren’t meant to be taken literally. For example, even an adult with autism might interpret a sarcastic “Oh, that's just great!” as meaning it really is great.
Conversely, someone affected by autism may not exhibit typical body language. Facial expressions, movements and gestures may not match what they are saying. Their tone of voice may fail to reflect their feelings. Some use a high-pitched sing-song or a flat, robot-like voice. This can make it difficult for others know what they want and need. This failed communication, in turn, can lead to frustration and inappropriate behavior (such as screaming or grabbing) on the part of the person with autism. Fortunately, there are proven methods for helping children and adults with autism learn better ways to express their needs. As the person with autism learns to communicate what he or she wants, challenging behaviors often subside.
Repetitive Behaviors
Unusual repetitive behaviors and/or a tendency to engage in a restricted range of activities are another core symptom of autism. Common repetitive behaviors include hand-flapping, rocking, jumping and twirling, arranging and rearranging objects, and repeating sounds, words, or phrases. Sometimes the repetitive behavior is self-stimulating, such as wiggling fingers in front of the eyes.
The tendency to engage in a restricted range of activities can be seen in the way that many children with autism play with toys. Some spend hours lining up toys in a specific way instead of using them for pretend play. Similarly, some adults are preoccupied with having household or other objects in a fixed order or place. It can prove extremely upsetting if someone or something disrupts the order. Along these lines many children and adults with autism need and demand extreme consistency in their environment and daily routine. Slight changes can be extremely stressful and lead to outbursts
Repetitive behaviors can take the form of intense preoccupations, or obsessions. These extreme interests can prove all the more unusual for their content (e.g. fans, vacuum cleaners or toilets) or depth of knowledge (e.g. knowing and repeating astonishingly detailed information about Thomas the Tank Engine or astronomy). Older children and adults with autism may develop tremendous interest in numbers, symbols, dates or science topics.
Associated Medical Conditions
Thanks to donor support, Autism Speaks continues to fund research into the causes and treatment of the medical conditions associated with ASD. You can explore these studies here. This research is reflected in the comprehensive care model at the heart of our Autism Treatment Network(ATN) clinics.
Genetic Disorders
Some children with autism have an identifiable genetic condition that affects brain development. These genetic disorders include Fragile X syndrome, Angelman syndrome, tuberous sclerosis and chromosome 15 duplication syndrome and other single-gene and chromosomal disorders. While further study is needed, single gene disorders appear to affect 15 to 20 percent of those with ASD. Some of these syndromes have characteristic features or family histories, the presence of which may prompt your doctor to refer to a geneticist or neurologist for further testing. The results can help guide treatment, awareness of associated medical issues and life planning.
Gastrointestinal (GI) Disorders
GI distress is common among persons with autism, and affects up to 85 percent of children with ASD. These conditions range in severity from a tendency for chronic constipation or diarrhea to inflammatory bowel disease. Pain caused by GI issues can prompt behavioral changes such as increased self soothing (rocking, head banging, etc) or outbursts of aggression or self-injury. Conversely, appropriate treatment can improve behavior and quality of life. Please see our treatment section on “Gastrointestinal Disorders.” It includes discussion of popular dietary interventions.
Seizure Disorders
Seizure disorders, including epilepsy, occur in as many as 39 percent of those with autism. It is more common in people with autism who also have intellectual disability than those without. Someone with autism may experience more than one type of seizure. The easiest to recognize is the grand mal, or tonic-clonic, seizure. Others include “petit mal” seizures (when a person temporarily appears “absent”) and subclinical seizures, which may be apparent only with electroencephalogram (EEG) testing.
Seizures associated with autism tend to start in either early childhood or adolescence. But they may occur at any time. If you are concerned that you or your child may be having seizures, it is important to raise the issue with your doctor for possible referral to a neurologist for further evaluation.
Sleep Dysfunction
Sleep problems are common among children and adolescents with autism and may likewise affect many adults.
Sensory Processing Problems
Many persons with autism have unusual responses to sensory input. They have difficulty processing and integrating sensory information, or stimuli, such as sights, sounds smells, tastes and/or movement. They may experience seemingly ordinary stimuli as painful, unpleasant or confusing.
Some of those with autism are hypersensitive to sounds or touch, a condition also known as sensory defensiveness. Others are under-responsive, or hyposensitive. An example of hypersensitivity would be the inability to tolerate wearing clothing, being touched or being in a room with normal lighting. Hyposensitivity can include failure to respond when one’s name is called. Many sensory processing problems can be addressed with occupational therapy and/or sensory integration therapy.
Pica
Pica is a tendency to eat things that are not food. Eating non-food items is a normal part of development between the ages of 18 and 24 months. However, some children and adults with autism and other developmental disabilities continue to eat items such as dirt, clay, chalk or paint chips. For this reason, it is important to test for elevated blood levels of lead in those who persistently mouth fingers or objects that might be contaminated with this common environmental toxin.
CAUSES
Source: http://www.nhs.uk/conditions/autistic-spectrum-disorder/pages/causes.aspx
Causes of autism spectrum disorder
The exact cause of autism spectrum disorder (ASD) is currently unknown.
It's a complex condition and may occur as a result of genetic predisposition (a natural tendency), environmental or unknown factors.
Genes
Most researchers believe that certain genes a child inherits from their parents could make them more vulnerable to developing ASD.
Cases of ASD have been known to run in families. For example, younger siblings of children with ASD can also develop the condition, and it's common for identical twins to both develop ASD.No specific genes linked to ASD have been identified, but it may be a presenting feature of some rare genetic syndromes, including Fragile X syndrome, Williams syndrome and Angelman syndrome.
Environmental triggers
Some researchers believe that a person born with a genetic vulnerability to ASD only develops the condition if they're exposed to a specific environmental trigger. Possible triggers include being born prematurely (before 35 weeks of pregnancy), or being exposed in the womb to alcohol or to certain medication, such as sodium valproate (sometimes used to treat epilepsy during pregnancy).
RISK FACTORS
Source: http://www.globalhealingcenter.com/natural-health/8-risk-factors-for-autism/
- Mycotoxins
- C-Sections
- Maternal Antibodies
- Placenta Abnormalities
- Smoking
- Air Pollution
- Endocrine Disruptors
- Vaccines
DIAGNOSIS
Source: http://www.nhs.uk/Conditions/Autistic-spectrum-disorder/Pages/Diagnosis.aspx
The specialist or specialist team will make a more in-depth assessment, which should be started within three months of the referral.
If you're referred to an individual specialist, they may be a:
- psychologist – a healthcare professional with a psychology degree, plus further training and qualifications in psychology
- psychiatrist – a medically qualified doctor with further training in psychiatry
- paediatrician – a doctor who specialises in treating children
Some local health authorities use multidisciplinary teams. These are a combination of specialists who work together to make an assessment.
Assessment
A diagnosis of ASD is based on the range of features your child is showing.
For most children:
- information will be needed from your GP, nursery or school staff, plus speech and language and occupational therapists, about your child's development, health and behaviour
- a speech and language therapist, and often an occupational therapist, will carry out an assessment
- a detailed physical examination will need to be carried out to rule out possible physical causes of your child's symptoms, such as an underlying condition like neurofibromatosis or Down's syndrome
- the assessment will include a check for any coexisting physical health conditions and mental health problems
- you may be asked to attend a series of interviews so a detailed family history and the history of your child's development and behaviour can be drawn up
- your child may be asked to attend a series of appointments so specific skills and activities can be observed and assessed
- Once this process is complete, a diagnosis of ASD may be confirmed.
- After diagnosis
- When a child is diagnosed with ASD, many parents are keen to find out as much as they can about the condition. The National Autistic Society has an excellent range of resources and advice.
TREATMENT
Source: http://www.nhs.uk/Conditions/Autistic-spectrum-disorder/Pages/Treatment.aspx
There's no 'cure' for autism spectrum disorder (ASD). However, a range of specialist educational and behavioural programmes can help children with ASD.
Any intervention should focus on important aspects of your child's development. These are:
- communication skills – such as using pictures to help communicate (as speech and language skills are usually significantly delayed)
- social interaction skills – such as the ability to understand other people's feelings and respond to them
- imaginative play skills – such as encouraging pretend play
- academic skills – the "traditional" skills a child needs to progress with their education, such as reading, writing and maths
- a paediatrician
- mental heath specialists, such as a psychologist and psychiatrist
- a learning disability specialist
- a speech and language therapist
- an occupational therapist
- education and social care services
- Parent education and training
- Psychological treatments
- Medication
EXTRA INFORMATION
Source: http://www.cdc.gov/ncbddd/autism/data.html
Data & Statistics
Prevalence
About 1 in 68 children has been identified with autism spectrum disorder (ASD) according to estimates from CDC's Autism and Developmental Disabilities Monitoring (ADDM) Network.
ASD is reported to occur in all racial, ethnic, and socioeconomic groups.
ASD is about 4.5 times more common among boys (1 in 42) than among girls (1 in 189).
Studies in Asia, Europe, and North America have identified individuals with ASD with an average prevalence of between 1% and 2%.
About 1 in 6 children in the United States had a developmental disability in 2006-2008, ranging from mild disabilities such as speech and language impairments to serious developmental disabilities, such as intellectual disabilities, cerebral palsy, and autism.